




Chiba Medical J. 94E:33-36,2018
doi:10.20776/S03035476-94E-3-P33
[ Original Article ]
Naoki Shimizu1), Osamu Saito1) and Nao Nishimura2)
1) Department of Pediatric Emergency & Critical Care Medicine, Tokyo Metropolitan Children’s Medical Center, Tokyo 183-8561.
2) Division of Critical Care Medicine, National Center for Child Health & Development, Tokyo 157-8535.
(Received April 27, 2018, Accepted May 9, 2018)
Transportation, whether by ground or air, exposes patients and health care providers to mechanical shocks, vibrations, and loud noises. The potential dangers posed by these forces remain largely unknown. We investigated the three dimensional vibration / acceleration forces during pediatric transportation in an ambulance and helicopter. The vibration / acceleration forces were almost 1 m/s2 during transport by helicopter including both takeoff and landing. However, transport by ambulance showed remarkable omnidirectional vibration often up to 2 m/s2 and sometimes reaching 3-4 m/s2. Further evaluation of vibrational stress and means of attenuating vibration during pediatric transportation are needed to enhance patient safety.
Children, Ground, Air, Acceleration, Stress
Interhospital transportation of sick and / or injured children is becoming more common due to the centralization of pediatric intensive care. Transportation, whether by ground or air, exposes patients and health care providers to mechanical shocks, vibrations, and loud noises. However, the hazardous nature of these forces remains largely unknown.
Vibration and noise are stressors that may adversely affect the well-being of children during transportation between facilities. Several studies have examined neonatal transportation[1-12], but little research has been done in pediatric transportation, and no studies in Japan have addressed this issue, let alone compared the impact of mechanical forces generated during ambulance and helicopter transport.
In the absence of evidence, many health care providers tend to believe that the ambulance generates less vibration / acceleration stress than the helicopter. This misconception may lead to a bias in the selection of transport method, with unforeseen consequences to the children being transported.
This study aimed to investigate three dimensional vibration / acceleration forces generated during pediatric transportation in an ambulance and a helicopter.
Pediatric transportation was done from Tokyo to Kyoto using both an ambulance and a helicopter. Due to the relatively large distance, the helicopter needed to be refueled at intervals. An ambulance was used for local destinations in the Kyoto area. The helicopter was flown from Aero Asahi, a landing area commonly used by medical helicopters. The ambulance in this study was the standard model used by the Japanese Fire Department.
The patient was loaded onto the back board with the pumps and monitors en bloc, in order to minimize the risk of accidents at take-off and landing. Three dimensional acceleration sensors were fixed onboard near the patient’s head. Vibration levels were measured continuously during the entire duration of transport. The X axis represents the left-to-right vibration forces, the Y axis represents between the back-and-forth vibration forces, and the Z axis represents the vertical vibration forces.
The data were analyzed after the transportation was completed. The taking of these measurements at no time compromised any clinical procedure or medical mission. Publication was approved by the Institutional Review Board of Tokyo Metropolitan Children’s Medical Center.
Table 1 shows the transport agenda. The patient was transported from the rooftop heliport of the children’s hospital in Tokyo to a heliport on the ground in Kyoto, with a midway refueling stop at Nagoya. After arrival in the helicopter, the patient was transferred to an ambulance and taken to the destination hospital. The traveling distance was over 450 km and required 3 hours and 13 minutes to cover.
Travel plan from Tokyo to Kyoto
The total transport data including the three dimensional acceleration forces are shown in Figure 1. The horizontal line represents time, and the vertical line represents the vibration / acceleration force(m/s2). Figure 2 shows the separate forces along the X(right to left), Y(back and forth), and Z(up and down) axes. Figure 3 shows each phase of the transportation including takeoff from the hospital roof, aerial transport by helicopter, landing on the ground, and ground transport by ambulance.
The vibration / acceleration forces were almost 1 m/s2 during air transportation including both takeoff and landing. On the other hand, travel by ambulance showed a high degree of omnidirectional vibration. The Z axis (up and down) showed stronger force overall at over 1 m/s2 during the entire duration of transportation, often reaching 2 m/s2 and sometimes even 3-4 m/s2. Additionally, boarding /disembarking from the helicopter and ambulance both showed strong vibrations of 4-5 m/s2.
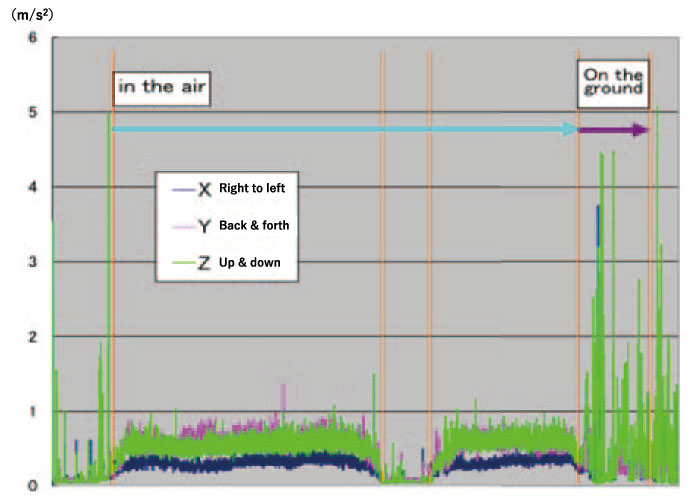
Figure 1
Total transport data including the three dimensional acceleration forces. The horizontal line represents time, and the vertical line represents the vibration / acceleration force(m/s2).
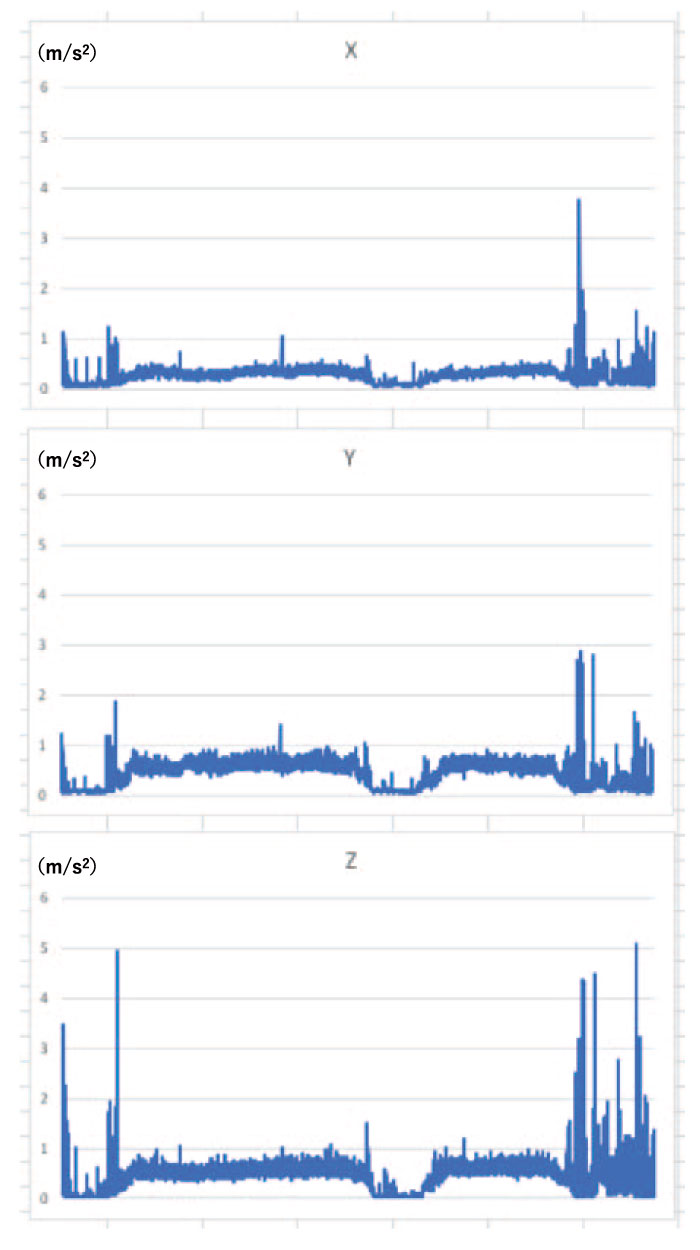
Figure 2
The separate forces along the X(right to left), Y (back and forth), and Z(up and down) axes.
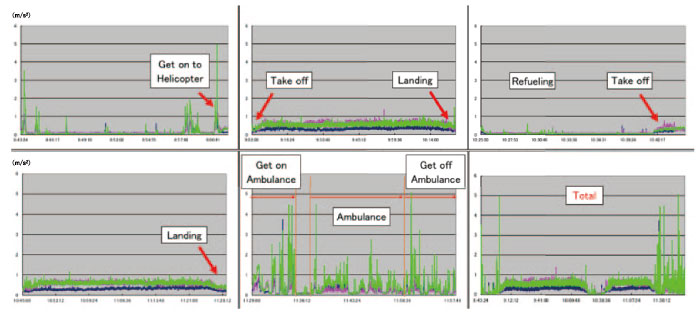
Figure 3
Each phase of the transportation including takeoff from the hospital roof, aerial transport by helicopter, landing on the ground, and ground transport by ambulance.
Despite the misconception that transport by helicopter involves stronger vibrations than by ambulance, our data showed that travel by helicopter was more stable even at takeoff and landing. During air travel, the vibrations along the X axis(right and left) were weak at around 0.5 m/s2. On the other hand, travel by ambulance showed remarkable instability in all dimensions as indicated in the results.
Vibrations in excess of 1.5 m/s2 are considered“ very uncomfortable,” and vibrations exceeding 2.0 m/s2 are considered“ extremely uncomfortable” by healthy adults [13]. Thus, transport by helicopter is more comfortable than by ambulance. Furthermore, the conditions described here may affect not only patients but also health care providers. While transporting pediatric patients, close attention must be given to ensure that several tubes including the end-tracheal tubes are maintained securely at the proper location and depth. Hence the strength of the vibration / acceleration force becomes a very important consideration when selecting a transport method.
A number of previous studies have reported different results from ours such as greater lateral and vertical forces during a helicopter landing[14]. Even so, headto- toe forces are weaker in a helicopter. The differences in the findings may be due to variations in the size of the helicopters studied or differences in specifications between Japanese and non-Japanese models. We also did not evaluate the differences in the sound, seating / work space for health care providers during transport, etc., all of which constitute limitations in this study.
Decreasing vibrations during pediatric interfacility transport may help to improve the safety of sick children during transport[13]. There are several studies indicating some benefit using water pillow for head stability, however, may cause opposite effect based on its resonance property. Further evaluation of vibration stress and finding the means of attenuating vibrations in pediatric transport vehicles are needed to enhance the safety of children during transport[15].
Although selection of vehicles, such as helicopter of ambulance, is usually based on the distance of transportation, the keys to successful pediatric air and land transport are the transport team’s knowledge of the physiological changes that may occur, their ability to assess the children’s physical state accurately, preventing stressors whenever possible, and properly intervening as necessary.
NS conceived and designed the study. OS is involved in data collection. NS, OS, and NN analyzed and interpreted the data, and were involved in development, review, and approval of the manuscript.
I would like to thank Mr. Dan Nitta of Metran Co., Ltd. for conducting the vibration / acceleration measurements and analyzing the data. I also would like to thank Mr. James Robert Valera for his assistance with editing the manuscript.
The authors declare that they have no conflicts of interest, either financial or non-financial, with the context of this article.
Address correspondence to Dr. Naoki Shimizu.
Department of Pediatric Emergency & Critical Care Medicine,
Tokyo Metropolitan Children’s Medical Center, 2-8-29,
Musashidai, Fuchu,Tokyo 183-8561, Japan.
Phone: +81-42-300-5111. Fax: +81-42-312-8160.
E-mail:naoki_shimizu@mac.com
