




Chiba Medical J. 94E:37-44,2018
doi:10.20776/S03035476-94E-4-P37
[ Original Article ]
Kazuhide Inage1), Sumihisa Orita1), Kazuki Fujimoto1),
Kazuyo Yamauchi1), Masao Koda2), Tsutomu Akazawa3), Yawara Eguchi4),
Takeo Furuya1), Junichi Nakamura1), Miyako Suzuki5),
Yoshihiro Sakuma6), Go Kubota7), Yasuhiro Oikawa8), Takeshi Sainoh9),
Jun Sato10), Yasuhiro Shiga1), Koki Abe1), Hirohito Kanamoto1),
Masahiro Inoue1), Hideyuki Kinoshita1), Masaki Norimoto1),
Tomotaka Umimura1), Kazuhisa Takahashi1) and Seiji Ohtori1)
1 ) Department of Orthopaedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670 .
2 ) Department of Orthopaedic Surgery, Faculty of Medicine, University of Tsukuba, Ibaraki 305-8575 .
3 ) Department of Orthopaedic Surgery, St. Marianna University School of Medicine, Kanagawa 216-8511 .
4 ) Department of Orthopaedic Surgery, Shimoshizu National Hospital, Yotsukaido 284-0003 .
5 ) Department of Bioenvironmental Medicine, Graduate School of Medicine, Chiba University, Chiba 260-8670 .
6 ) Department of Orthopaedic Surgery, National Hospital Organization, Chiba Medical Center, Chiba 260-8606 .
7 ) Department of Orthopaedic Surgery, Eastern Chiba Medical Center, Togane 283-8686 .
8 ) Department of Orthopaedic Surgery, Chiba Children’s Hospital, Chiba 266-0007 .
9 ) Department of Orthopaedic Surgery, Sainou Hospital, Toyama 930-0866 .
10 ) Department of Orthopaedic Surgery, Chiba Aoba Municipal Hospital, Chiba 260-0852 .
(Received January 23, 2018, Accepted March 15, 2018)
Purpose. To compare compression and ice treatments in a rat model of muscle injury.
Methods. A model of muscle injury was made in 108 eight-week-old Sprague Dawley male rats by dropping a weight onto their right gastrocnemius muscle. We compared compression and ice treatments after the contusion injury with no treatment. We evaluated the injuries using histology and an enzyme-linked immunosorbent assay for tumor necrosis factor α. We used Fluoro-Gold to trace neural afferents from the region of the contusion injury. The proportion of calcitonin gene-related peptide-immunoreactive neurons in all Fluoro-Gold-labeled neurons was determined to evaluate pain.
Results. In the compression treatment group, the injured muscle tended to have less hemorrhage and edema at ≥ 6 h after the injury. Tumor necrosis factor α levels were lower, and the local acutephase inflammatory reaction was milder than in untreated rats. We found less necrosis of muscle tissue on the third day after injury and the replacement of granulation tissue and regeneration of muscle fibers 1 week after the injury. The proportion of calcitonin gene-related peptide-immunoreactive Fluoro-Gold-labeled neurons in total Fluoro-Gold-labeled neurons was significantly lower than in untreated rats.
In the ice treatment group, although injured muscle had decreased hemorrhage and edema 6 h after the injury, hemorrhage and edema increased ≥18 h after injury. Tumor necrosis factor α levels were transiently increased compared with those in untreated rats( 3 h and 6 h after contusion). On the third day after contusion injury, necrosis of muscle was severe. We observed the replacement of granulation tissue and regeneration of muscle fibers 1 week after the injury. The proportion of calcitonin gene-related peptide-immunoreactive Fluoro-Gold-labeled neurons was significantly lower than in untreated rats.
Conclusion. In our study, compression may promote muscle tissue repair by preventing hematoma formation during the repair phase and preventing prolonged pain. On the other hand, ice therapy may prevent prolonged pain through pain relief from the stimulation of cold receptors, enabling animals to proceed with an early range of motion exercise, suppressing hypoactivity and promoting muscle tissue repair during the recovery phase. Overall, our current study indicated that there was a difference between compression and ice treatments during the acute and repair phases of muscle injury.
muscle injury, compression treatment, ice treatment, rat
Muscle injuries account for 10%-55% of sportsrelated external injuries and strains and contusions are common among muscle injuries[1]. Muscle contusion is a condition where muscle fibers become damaged by an external force, and frequently occurs on the front side of the femoral region; this injury is often observed in sports such as soccer, rugby, and American football. Treatment including rest, ice, compression, and elevation(RICE) can generally be provided during the acute phase of therapy in clinical practice. In particular, compression and ice are widely used at clinical sites as an emergency treatment. Hematoma can be suppressed by local compression, but the appropriate treatment period remains unknown. Ice treatments require a number of applications; however, the most appropriate time to initiate treatment and the optimal treatment period remain unknown[2-4]. Only a few reports have described the mechanism of compression and ice therapies in any detail. Therefore, in the current study, we examined and compared the effect of compression and ice treatment in a rat model of muscle injury repair.
All the animal procedures and protocols were approved by the ethics committee of our university and followed the U.S. National Institutes of Health Guidelines for the Care and Use of Laboratory Animals (1996 revision). We used 108 eight-week-old male Sprague Dawley rats. Each rat weighed approximately 250 g at the time of muscle injury. Before inducing the injury, the rats were anesthetized with ethyl ether. If a withdrawal reflex occurred, additional anaesthesia was administered until no response was noted. The muscle injuries were induced without making a skin incision. Muscle contusion injury was achieved by dropping a 115g weight 1 m onto an impactor placed on the right medial gastrocnemius muscle[5](Fig. 1). The gastrocnemius muscle of the left leg was used as a control. We examined and compared the following three groups within 3 h of the contusion injury(Fig. 2): a compression treatment group(n=36 rats), the region of the contusion injury was compressed with latex rubber(300 mmHg compression for 30 min); an ice therapy group(n=36 rats), in which the region of the contusion injury was packed with ice(30 g) for 30 min; and a group without treatment(n=36 rats).
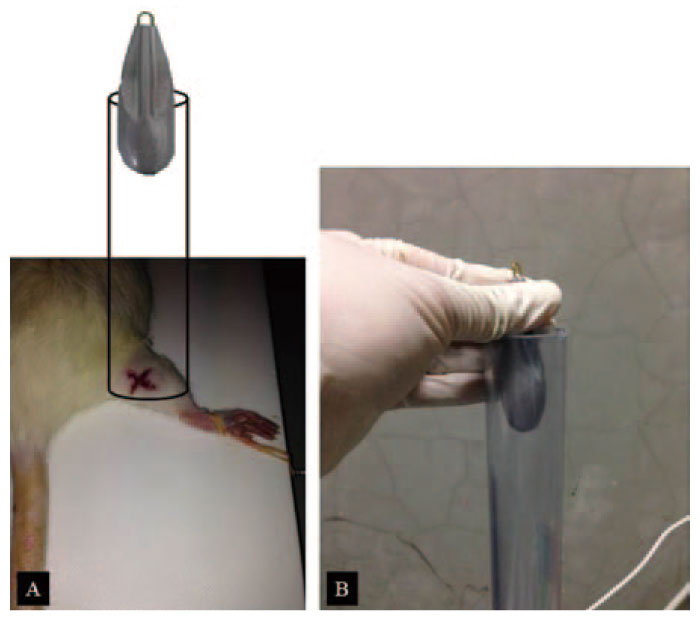
Fig. 1
The drop-mass method.(A) Schematic of the impact apparatus. (B) A 115-g weight was dropped 1 m through an acrylic guide tube. The weight dropped onto an impactor, driving it into the muscle belly causing a contusion injury without penetrating the overlying skin.
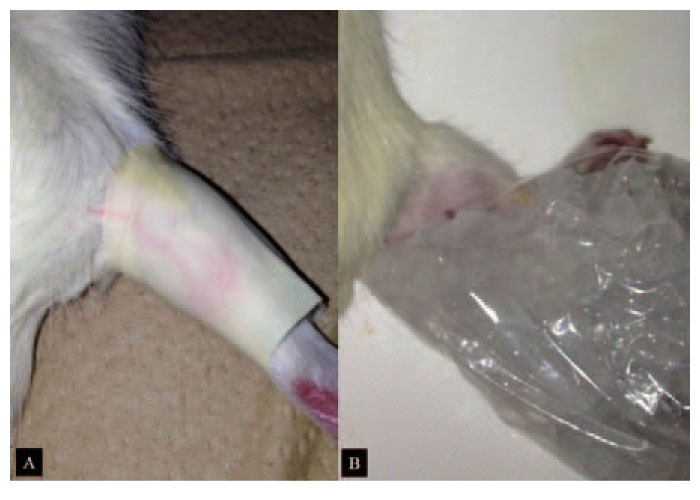
Fig. 2
(A) The compression therapy group in which the region of the contusion injury was compressed with latex rubber(300 mmHg compression for 30 min).(B) The ice therapy group in which the region of the contusion injury packed with ice(30 g) for30 min.
After anesthesia with sodium pentobarbital(40 mg/kg, intraperitoneally) at 3 h, 6 h, 18 h, 24 h, 3 days, 1 week, and 2 weeks after the muscle injury rats(21; 3 per time point) were perfused transcardially with 0.9% saline followed by 500 mL of 4% paraformaldehyde in phosphate buffer(0.1 M, pH 7.4), and the muscle injury sites(right sides) in each of the three groups were dissected from the hind limbs. Each formalin-fixed tissue specimen was embedded in a paraffin block after dehydration for 14 h using an ascending series of ethanol concentrations in a Tissue-Tek vacuum infiltration tissue processor(M1500; Sakura Finetek Japan Co, Tokyo, Japan). Sections(4 μm) were prepared from these paraffin blocks using a sliding microtome(LS113; Yamato-Kohki Industrial Co, Saitama, Japan) and were mounted onto glass slides(No. 5116; Muto Pure Chemicals Co, Tokyo, Japan). The sections were stained with Mayer’s hematoxylin(Muto Pure Chemicals Co, Tokyo, Japan) for 5 min after deparaffinization with xylene and ethanol. After washing with distilled water, these sections were dipped in 0.1% ammonium solution several times, were washed again through a series of ethanol concentrations to 100%, and were stained with 1% eosin and phloxine solution for 20 s. Finally, they were covered with mounting medium(Entellan New; Merck, Darmstadt, Germany) after dehydration through a series of ethanol and xylene solutions. The sections were observed under a microscope(BH20; Olympus Corporation, Tokyo, Japan) by a professional animal pathologist, and the each finding was evaluated semiquantitatively. We evaluated the presence or absence of histological degeneration, bleeding, and neutrophil recruitment in each section, and compared the histological changes between the 3 groups.
Tissue levels of tumour necrosis factor(TNF)-α, an inflammatory mediator, were assayed in rat muscle tissue from each group at 3, 6, 18, and 24 h after muscle injury. Resected gastrocnemius muscle samples were frozen in liquid nitrogen, pulverized or homogenized, and digested in a tissue lysis reagent. TNF-α production at the muscle injury sites was quantified using an enzyme-linked immunosorbent assay (ELISA) in accordance with the manufacturer’s protocols(R&D Systems, Minneapolis, MN, USA). The tissue protein levels were assayed using a kit in accordance with the manufacturer’s protocols (Bio-Rad, Hercules, CA, USA), and the TNF-α levels were normalized to tissue protein levels.
Fluoro-Gold(FG), a retrograde neuronal tracer, was placed at the region of the contusion injury to label neural afferents. L4 dorsal root ganglia(DRG) were removed on the third day after the contusion injury; according to a previous report, the gastrocnemius muscle shows a significantly high proportion of L4 control. The proportion of FG-positive neurons also showing immunoreactivity (ir) for calcitonin gene-related peptide(CGRP), a marker of inflammatory pain, was determined. Endogenous tissue peroxidase activity was quenched by soaking sections in 0.3% hydrogen peroxide solution in 0.01 M phosphate-buffered saline (PBS) for 30 min. Specimens were then treated for 90 min at room temperature in a blocking solution consisting of 0.01 M PBS containing 0.3% Triton X-100 and 3% skim milk. The sections were labeled using a primary rabbit antibody to CGRP(Chemicon, Temecula, CA, USA) diluted 1: 1000 in blocking solution, and incubated for 20 h at 4 ℃. To detect CGRP-ir in DRGs, sections were incubated with goat anti-rabbit Alexa Fluor 488 fluorescent antibody conjugate(1: 400; Molecular Probes, Eugene, OR, USA). Sections were examined using a fluorescence microscope, and the number of FG-labeled neurons, total numbers of CGRPimmunoreactive neurons, and FG-labeled and CGRPimmunoreactive neurons were counted. A randomized sample of 10 areas of each section of DRG was counted.
Between group comparisons were evaluated using nonrepeated analysis of variance (ANOVA), with Bonferroni post-hoc correction for multiple comparisons. The level of significance was defined a priori as p<0.05.
The time-dependent changes in the histology of muscle samples from the 3 groups are shown in Figure 3.
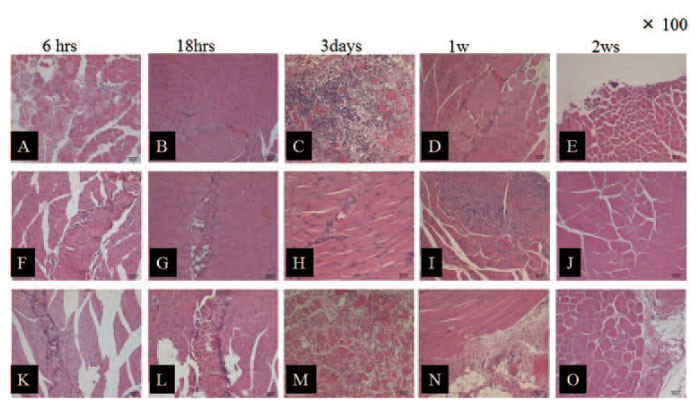
Fig. 3
Hematoxylin and eosin staining of the local tissues. Transverse sections showing the gastrocnemius muscle fibres(×100). The no treatment group at(A) 6 h;(B) 18 h;(C) 3 days;(D) 1 week; and(E) 2 weeks. The compression treatment group at(F) 6 h;(G) 18 h;(H) 3 days;(I) 1 week; and(J) 2 weeks. The ice treatment group at(K) 6 h;(L) 18 h;(M) 3 days;(N) 1 week; and(O) 2 weeks.
Hemorrhage and edema tended to be lower in the compression treatment group than in the untreated group, and these conditions were rarely observed on the third day post-injury in the compression treatment group. And the tissue repair process was initiated at the same time as that in the untreated group, while neutrophilic infiltration peaked at 6 h post-injury. The proliferation of fibroblast cells and macrophages was observed 18 h post-injury, which was similar to that in the untreated group. However, minimal necrosis of the muscle tissue was observed on the third day post-injury in the compression treatment group compared to that in the untreated group. The replacement of granulation tissue and regeneration of muscle fibers were observed in the first week post-injury, and the muscle fibers were mostly regenerated by the second week. Although neutrophilic infiltration peaked at 6 h post-injury and the proliferation of fibroblast cells and macrophages was observed 18 h post-injury in the compression group, the levels tended to be slightly high. Extensive necrosis of the muscle tissue was observed on the third day post-injury, which was similar to that observed in untreated rats. The replacement of granulation tissue and regeneration of muscle fibers were observed in the first week post-injury, and the muscle fibers were mostly regenerated by the second week post-injury, which was similar to the regeneration observed in the untreated treatment group.
Hemorrhage and edema were lower immediately after treatment(6 h post-injury) in the ice treatment group than in the untreated group. However, hemorrhage and edema conversely increased at 18 h and 24 h postinjury, respectively. The tissue repair process was apparently initiated as same time as that in untreated group. Neutrophilic infiltration reached a peak at 6 h post-injury, and proliferation of fibroblast cells and macrophages was observed 18 h post-injury. However, necrosis of the muscle tissue was observed extensively on the third day post-injury. In addition, residual necrosis was recognized 1 wk post-injury; however, there was a low amount of granulation-like tissue. Residual necrotic tissue was observed 2 wk post-injury; however, only partial regeneration of the muscle fiber was observed.
We found time-dependent changes in the TNF-α levels of the injured muscle tissue among the 3 groups (Fig. 4). In the untreated group, TNF-α levels peaked at 18 h post-injury and then decreased.
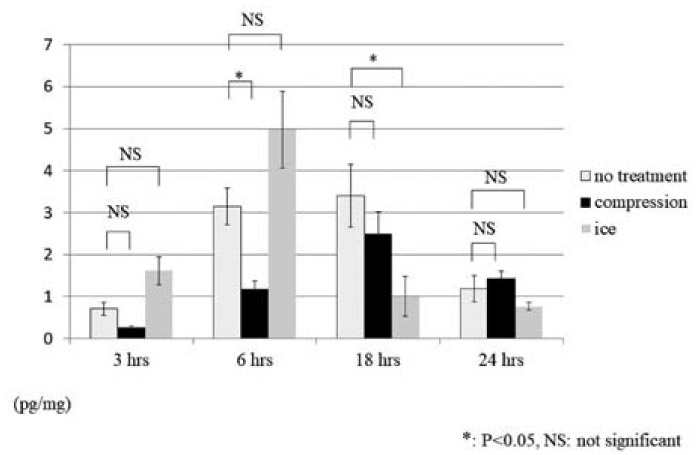
Fig. 4
The tumour necrosis factor-α levels in the muscle injury sites at 3, 6, 18, and24 h after muscle injury in the 3 groups.
In the compression treatment group, TNF-α levels showed a time-dependent change similar to that found in the untreated group; however, the levels at 3, 6, and 18 h post-injury were lower in the compression treatment group than in the untreated group. Particularly, the TNF-α levels at 3 and 6 h post-injury were significantly lower(3 h, P=0.071; 6 h, P=0.011). There was no significant difference in the TNF-α levels between the compression treatment group and untreated group 24 h post-injury( P=0.481).
TNF-α levels immediately after treatment(3 h postinjury) were higher in the ice treatment group than in the untreated group(P=0.0722); however, the levels significantly decreased 18 h post-injury(P=0.049). There was no significant difference in the TNF-α levels between the ice treatment group and untreated group 24 h post-injury(P=0.389).
L4 DRG immunohistochemistry is shown in Figure 5. The proportion of CGRP-ir FG-positive neurons was significantly lower in the compression treatment group and ice treatment group compared with the untreated group (compression therapy group, P=0.004; ice therapy group, P=0.0007). There was no significant difference between the treatment groups(P=0.485)(Fig. 6).
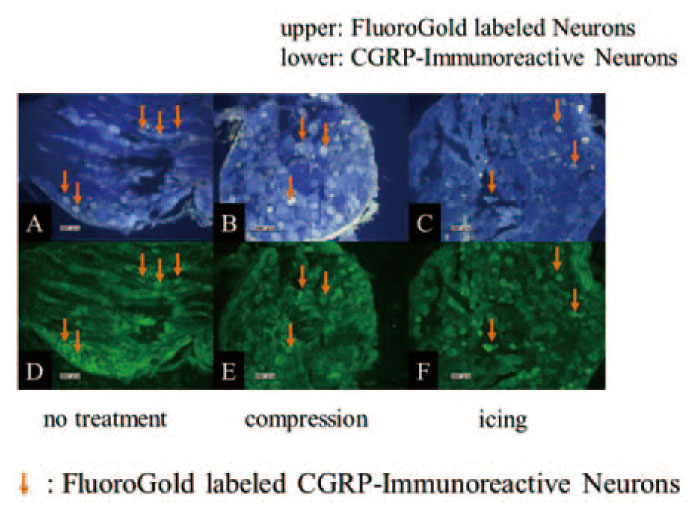
Fig. 5
The arrows indicate calcitonin gene-related peptide(CGRP)-immunoreactive Fluoro-Gold (FG)-labeled neurons.(A) FG-labeled neurons in the no treatment group; (B) FG-labeled neurons in the compression treatment group;(C) FG-labeled neurons in the ice treatment group; (D) CGRP-immunoreactive neurons in the no treatment group; (E) CGRP-immunoreactive neurons in the compression treatment group; and (F) CGRP-immunoreactive neurons in the ice treatment group.
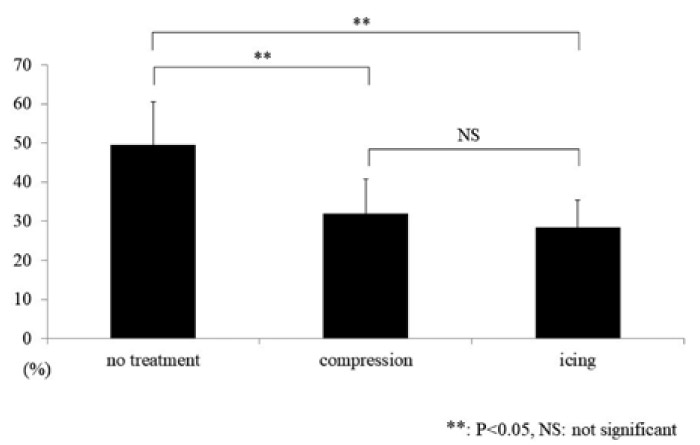
Fig. 6
In the L4 dorsal root ganglion, the proportion of calcitonin gene-related peptide immunoreactive Fluoro-Gold (FG) positive neurons in the compression treatment, ice treatment, and untreated groups.
In the compression treatment group, hemorrhage and edema tended to be less ≥ 6 h after the contusion injury. The muscle TNF-α levels were lower and the local acute-phase inflammatory reaction was milder compared with the untreated group. Compression treatment suppresses hemorrhage and edema in tissue and prevents secondary damage(e.g., necrosis) of surrounding tissue[6]. Early treatment by compression can be effective for suppressing a local acute-phase inflammatory reaction. Conversely, hemorrhage and edema were decreased 6 h after the contusion injury treated with ice, but the hemorrhage and edema were increased ≥18 h after the injury. TNF-α was transiently increased immediately after the compression treatment intervention compared with the untreated group(3 h and 6 h after the contusion injury). Ice treatment causes transient vasoconstriction, suppressing edema and hemorrhage. However, ice treatment leads to later vasodilatation and causes effects similar to those seen after thermal treatment[7]. Therefore, ice treatment transiently reduces hemorrhage and edema because of its vasoconstrictive action, but it was suggested that ice treatment later poses a risk by promoting a local acute-phase inflammatory reaction by having an effect similar to that seen after thermal treatment.
In the compression treatment group, we found less necrosis of rat muscle tissue on the third day after injury. We observed the replacement of granulation tissue and the regeneration of muscle fibers 1 week after the contusion injury. Furthermore, the proportion of CGRPir FG-positive DRG neurons was significantly lower than in untreated rats. The proportion of CGRP-ir FGpositive neurons has been reported to reflect prolonged pain. Compression treatment can be effective for muscle tissue repair, and to diminish prolonged pain. Hematomas can largely influence prolonged pain after muscle damage and can delay tissue repair[8]. It was considered that early treatment with compression would promote muscle tissue repair and prevent prolonged pain by preventing hematoma formation during the repair phase.
Conversely, necrosis of muscle on the third day after the contusion injury was seen to be severe after ice treatment, but the replacement of granulation tissue and the regeneration of muscle fibers was recognized 1 week after the injury. Furthermore, the proportion of CGRPir FG-positive neurons was significantly lower. This may be caused by a temporary hypoalgesic effect from the ice treatment. Analysis of somatosensory evoked brain potentials after noxious CO2 laser stimulation[9] suggests ice treatment would provide a pain relief effect by stimulation of cold receptors. Exacerbation of pain is considered suppressed by ice treatment; therefore, the proportion of CRGP-ir FG-positive neurons is significantly lower. The severe necrosis of muscle on the third day after injury is considered the result of not being able to maintain a healthy condition by suppressing hypoactivity along with pain relief by comparison with the untreated group. By contrast, an early range of motion exercise could be important for repairing muscle[10]. Therefore, it is considered that the regeneration of muscle fiber occurred 1 week after muscle injury, due to a suppression of hypoactivity that enables animals to proceed to an early range of motion exercise because of the pain relief afforded by the ice treatment.
There is a serious limitation in this study. That is, in this study, both treatment interventions are performed only one time immediately after injury. As mentioned in the introduction, the period and start time for both compression therapy and cooling therapy are unclear in actual clinics. Therefore, in the future, we plan to conduct research by changing the period and start time using this model.
In the current study, we examined and compared the effect of compression and ice treatment on muscle injury using a rat model. Our study suggests that compression treatment will suppress edema and hemorrhage of tissue during the acute phase of injury and that it can be a valid treatment for the suppression of local acute-phase inflammation. Compression may promote muscle tissue repair by preventing hematoma formation during the repair phase and preventing prolonged pain. By contrast, ice treatment may transiently reduce hemorrhage and edema because of a vasoconstriction effect, but it was also suggested that ice treatment later poses a risk that conversely promoted local acute-phase inflammation by showing an effect similar to that seen after thermal treatment. Ice therapy may prevent prolonged pain through pain relief from the stimulation of cold receptors, enabling animals to proceed with an early range of motion exercise, suppressing hypoactivity and promoting muscle tissue repair during the recovery phase. Overall, our current study indicated that there was a difference between compression and ice treatments during the acute and repair phases of muscle injury.
KI, SuO, KF, KY, MS, YoS, GK, YO, TS, JS, YaS and SeO designed research, analyzed and/or interpreted the data. KI, FK, TS, JS, YaS, KA, HK, MI, HK, MN and TU performed experiments. KI wrote the article and SuO, MK, TA, YE, TF, JN, MS, KT and SeO gave critical comments on the draft of the manuscript. All authors read and approved the final version of the manuscript.
The authors declare that they have no conflicts of interest, either financial or non-financial, with the contents of this article.
Address correspondence to Dr. Kazuhide Inage.
Department of Orthopaedic Surgery, Graduate School of Medicine, Chiba University,
1-8-1, Inohana, Chuou-ku, Chiba 260-8670, Japan.
Phone: +81-43-226-2117. Fax: +81-43-226-2116.
E-mail:kazuhideinage@yahoo.co.jp
