




Chiba Medical J. 94E:55-59,2018
doi:10.20776/S03035476-94E-6-P55
[ Case Report ]
Hiroakira Terakawa, Junichi Nakamura, Masahiko Sugano, Shigeo Hagiwara
Yasushi Wako, Michiaki Miura, Yuya Kawarai, Kento Nawata
Kensuke Yoshino, Sumihisa Orita, and Seiji Ohtori
Department of Orthopaedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670 .
(Received June 14, 2018, Accepted July 10, 2018)
Introduction: It is generally believed that total hip arthroplasty(THA) is contraindicated in Charcot arthropathy because of poor outcome. We describe a patient with Charcot arthropathy of the hip with a two-year follow-up after THA.
Case report: A 59-year-old woman with Charcot-Marie-Tooth disease complained of a sense of discomfort in her right hip joint and gait disturbance. X-ray imaging revealed disappearance of the right femoral head because of joint destruction. THA was conducted under a diagnosis of Charcot arthropathy. To prevent postoperative dislocation, a tractional direct anterior approach was applied to preserve the remaining muscle strength with a minimally invasive technique providing quick rehabilitation. Three dimensional, CT-based preoperative planning was used to achieve a safe zone for the implant alignment.
Conclusion: At two years after the THA, the outcome in this patient with Charcot’s arthropathy is satisfactory.
Charcot arthropathy, Charcot Marie Tooth disease, Total hip arthroplasty, Hip joint
Charcot arthropathy is a degenerative condition of the joints secondary to a neurological disturbance of analgesia, resulting in deformity and increased bone reabsorption[1]. This can strike patients with neurological conditions such as diabetes mellitus, syringomyelia, and other pathologies that have in common the alteration of sensitivity, not necessarily epicritic, but simply protopathic or deep sensitivity. This pathology introduces an arthrosis with severe joint destruction, particularly of the knee, hip, and foot. The patients have few clinical signs, but characteristic radiographic aspects include serious bony reabsorption, leading to articular destruction. The joint destruction progresses for a few months with some diagnostic problems. Even if the patients are asymptomatic, the deformity becomes visible[2]. It is generally considered that total hip arthroplasty(THA) is contraindicated in a Charcot joint[3-6]because of a few reports of recurrent dislocation and inevitable sequelae of implant loosening. However, advances in medicine have brought successful long-term outcomes of THA in patients with hip disease. We report a case of successful THA in one patient with Charcot joint of the hip caused by Charcot-Marie-Tooth disease(CMT).
A 59-year-old woman suffering from CMT felt a sense of discomfort in her right hip joint for 6 months. She had no history of trauma, malignancy, or infection. She could not walk without crutches. Detailed neurological examination subsequently revealed a distinct loss of vibratory sensibility and proprioception in her distal extremities bilaterally, but with intact pain and light touch sensation. Her hip pain was evident during joint motion or weight bearing. Mild muscle weakness of her distal extremities bilaterally was also observed. Her Japanese Orthopedic Association hip score was 59 points. She had undergone ankle arthrodesis bilaterally for club foot. Radiographs of the pelvis were examined because of the progressive gait disturbance. X-ray imaging revealed the disappearance of the right femoral head and leg length discrepancy(Fig. 1a). Computed tomography(CT) of the pelvis showed severe destruction of the proximal femur and acetabulum(Fig. 1b-e).
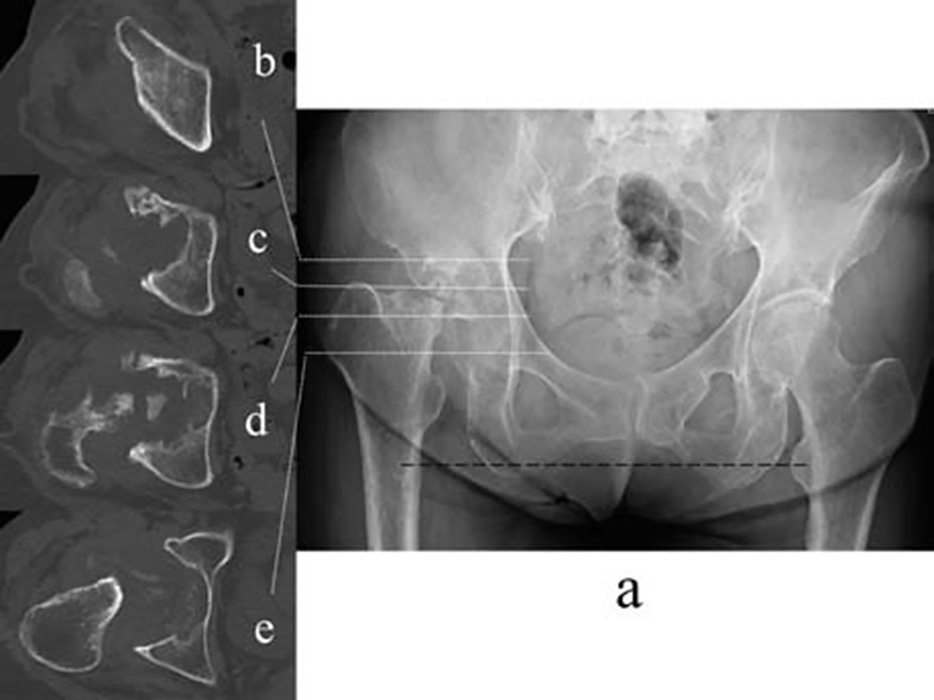
Fig. 1 Imaging features of the pelvis at the first visit.
Anteroposterior X-ray image shows severe joint destruction of the right hip with disappearance of the femoral head and the right femoral shortening followed by leg length discrepancy (horizontal reference line passing the left lesser trochanter in black broken line)(a). Computed tomography reveals destruction of the acetabulum at the: roof(b), joint line(b), center of the acetabulum(c), and tear drop(d).
We diagnosed Charcot arthropathy because of CMT and planned THA to recover her ability to walk. To prevent postoperative dislocation, a tractional direct anterior approach(DAA) in a supine position was applied to preserve the remaining muscle strength with this minimally invasive technique providing quick rehabilitation. Three dimensional, CT-based preoperative planning(ZedHip, Lexi, Tokyo, Japan) was performed to achieve a safe zone of implant alignment[7](Fig.2). A cementless acetabular cup and highly crosslinked polyethylene liner(R3, Smith and Nephew, Memphis, TN) were applied. A cementless femoral stem of Zweymuller type with a modular neck(ProfemurZ, Microport, Arlington, TN) and ceramic head(Biolox Delta, Ceramtec, Plochingen, Germany) were applied. Both the cup and stem achieved a good press-fit stability. Then, anterior and posterior stabilities were checked to select the most suitable femoral neck length, off-set, neck angle, and shape of polyethylene liner. Ultimately, a straight-short neck, 32 mm small head, and flat liner were determined.
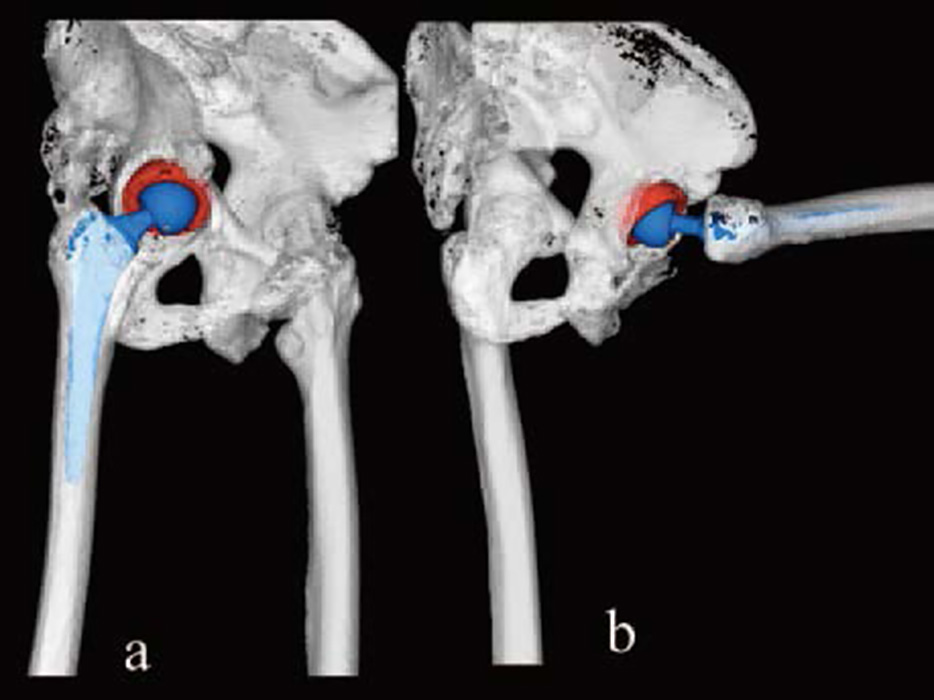
Fig. 2 Three dimensional, CT-based preoperative planning of total hip arthroplasty.
Anterior dislocation is simulated by 10° of extension and 42° of external rotation(a). Posterior dislocation is simulated by 90° of flexion and 12° of internal rotation(b).
Pathological examinations revealed nonspecific necrosis and chronic reactive changes of bone and soft tissue, without cultures for bacteria, fungi, or acidfast bacilli. Rehabilitation began on postoperative day one with full weight bearing. On postoperative day 14, the patient was discharged to a rehabilitation facility followed by regular physical therapy at an outpatient clinic. Postoperative evaluation of the implant alignment with three dimensional, CT-based software showed excellent alignment(Fig. 3). At two years after the THA, her hip joint functioned flawlessly without dislocation and X-ray imaging showed the implants were stable(Fig. 4). The patient was satisfied with the surgical outcome of 83 points by Japanese Orthopaedic Association Hip score(pain 40 points, flexion 9 points, abduction 5 points, gait 15 points, and activity of daily living 14 points).
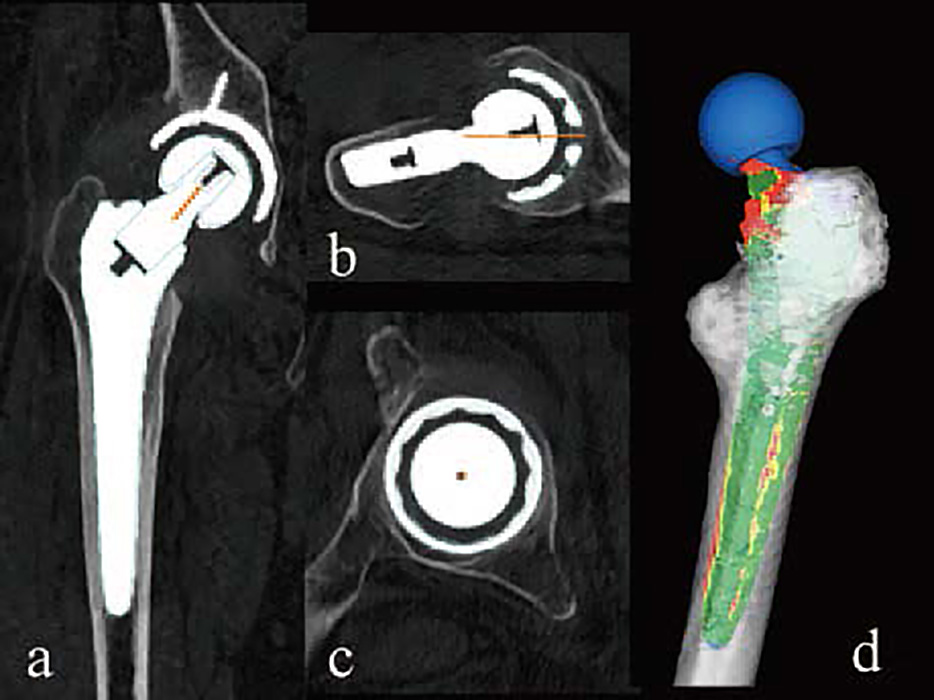
Fig. 3 Postoperative evaluation of implant alignment with three dimensional, CT-based software.
Coronal reconstruction(a), oblique axial reconstruction of the femoral neck(b), oblique sagittal reconstruction of the cup(c) shows 33° of cup radiographic inclination, 13° of radiographic anteversion, 15° of stem anteversion, and 27° of combined anteversion(postoperative templating in blue). Three dimensional, canal filling analysis indicates that the edges along the square stem fit well in yellow and red.
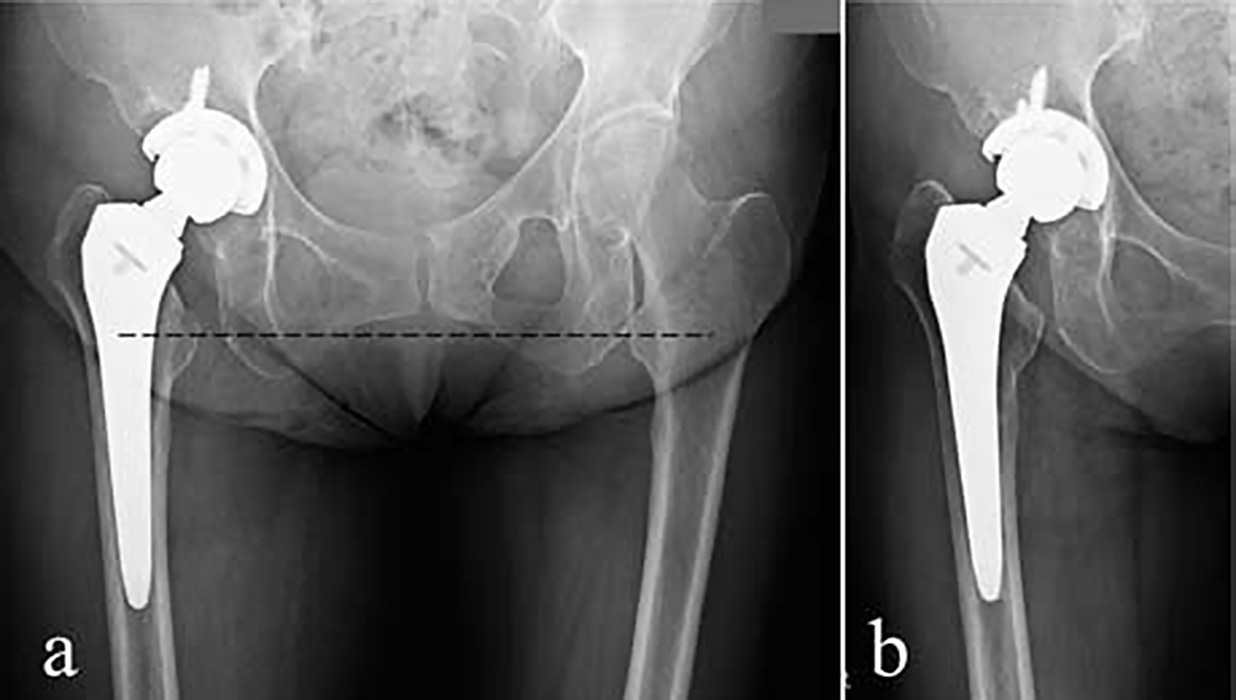
Fig. 4 X-ray images of the right hip during two years follow-up.
Immediately after surgery, the implants are well fixed in excellent alignment without leg length discrepancy(horizontal reference line passing the left lesser trochanter in black broken line)(a). An X-ray image taken two years later shows no evidence of loosening or dislocation of the implants(b).
CMT is one of the most common inherited neuropathies with an estimated prevalence of one in 2,500. CMT is a disorder of the peripheral nerves that causes progressive distal to proximal weakness and associated atrophy and sensory deficits, usually affecting the feet and legs at onset[8]. Charcot joint is a neurogenic arthropathy that can strike patients with deficit of the superficial and deep sensitivity [2]. In 1868, Jean-Martin Charcot[9]gave the first description of the neuropathic aspect of this joint. Although in most patients neuropathic aspects are associated with diabetic neuropathy, they may show spine or peripheral nerve damage, neurosyphilis, alcoholism, or vitamin deficiency. Two main theories predominate in the pathophysiology of neuropathic osteoarthropathy. The neurotraumatic theory states that the arthropathy is caused by an unperceived trauma or injury to an insensitive functional joint. The second theory is the neurovascular theory, which suggests that the development of autonomic neuropathy causes an increased blood flow to the joint; this in turn results in a mismatch in bone destruction and regeneration, leading to joint hypertrophy and architectural distortion[10]. It is likely that a combination of these two processes plays a role in the development of a Charcot joint. Imaging studies typically show extensive bone reabsorption, heterotopic ossification and fibrosis, periarticular bony debris, and soft-tissue inflammation. Misdiagnosis as osteomyelitis or a neoplasm is frequent[11].
Surgical treatment for neuropathic arthropathy of the hip is controversial. Historically, arthrodesis was a preferred strategy for management even with high failure rates after hip fusion[8,12]. THA had been discouraged as a result of various reviews reporting on the negative results of THA for a Charcot joint, which are mostly complications of recurrent dislocation and implant loosening[4-6,13]. The causes of failure are likely to be laxity of the joint capsule and ligaments, and muscle weakness for dislocation, and bone absorption around the implant because of material failure as a result of poor quality polyethylene or surface finishing of the implant. However, recent advances in medicine encourages successful long-term outcome of THA in patients with hip disease. In some cases, artificial joint replacement achieved positive results for Charcot hip arthropathy. Rapała and Obrębski[14]reported a successful 10-year result of THA, and Sprenger and Foley[15]described a case of successful outcome of THA in a preataxic patient with Charcot hip.
To avoid dislocation, we used three strategies. First, we ensured precise preoperative planning using three dimensional, CT-based software. This software can simulate postoperative ROM of the hip and display the position of impingement. Thereby, the risk of impingement of implant can be reduced and a safe zone of the implant alignment can be achieved. Second, we applied a tractional DAA to preserve the remaining muscle strength with this minimally invasive technique. A DAA exposes the true intermuscular and internervous plane and is muscle sparing of the gluteus medius and minimus, and the gluteus maximus and the tensor fascia lata, which serve as hip abductors and pelvic stabilizers [16]. Preservation of the posterosuperior capsule or the short external rotators results in a low rate of dislocation for a tractional DAA[17]. Third, we selected a modular neck stem. In this system, the most stable combination of the femur neck length and neck angle can be confirmed by soft tissue tension through an anterior and posterior stability test. These strategies have achieved a successful THA at two-year follow-up in the present patient.
All authors contributed to patient management and writing of the report. Written consent was obtained from the patient for publication of this case report and accompanying images.
The corresponding author, Junichi Nakamura, was supported by JSPS KAKENHI grant number 17K10954 and Takeda Science Foundation.
Address correspondence to Dr. Junichi Nakamura.
Department of Orthopaedic Surgery, Graduate School of Medicine, Chiba University, 1-8-1, Inohana, Chuou-ku, Chiba 260-8670, Japan.
Phone: +81-43-226-2117. Fax: +81-43-226-2116.
E-mail: njonedr@chiba-u.jp
Abbreviations: Total hip arthroplasty(THA), Charcot Marie Tooth Disease(CMT), Direct Anterior Approach(DAA)
