




Chiba Medical J. 94E:65-67,2018
doi:10.20776/S03035476-94E-6-P65
[ Case Report ]
Naoki Shimizu1), Eri Mineo1,2), Tadashi Kodani1), and Osamu Saito1)
1 ) Department of Pediatric Emergency & Critical Care Medicine, Tokyo Metropolitan Children’s Medical Center,Tokyo 183-8561 .
2 ) Department of Pediatrics, Kitasato University, Kanagawa 252-0375 .
(Received May 10, 2018, Accepted August 1, 2018)
Human parechovirus(HPeV), a potentially severe viral infection in infants and one of the chief causes of fever in young infants, typically presents fever, irritability, and rash, thus accounting for the patients’ being described as“ hot, red, angry babies”. Treatment is primarily supportive and includes management of complications. Some infants with a severe HPeV infection may suffer adverse neurodevelopment, and follow-ups by a pediatrician are recommended. We experienced an infantile case of HPeV infection requiring critical care in which the interleukin-6 levels was not elevated. The immune response in HPeV infections is not fully understood and requires further study for clarification.
Severe sepsis, Septic shock, Interleukin, Cytokine, Picornaviridae
Human parechovirus (HPeV) is an important cause of fever in young infants, who characteristically present with fever and irritability and occasionally also present a diffuse rash[1]. The severe form of the disease can lead to meningoencephalitis, seizure, sepsis-like presentations including septic shock as well as less common presentations including signs of surgical abdomen[2-7]. There are no effective antiviral therapies. Treatment is primarily supportive and includes management of complications. Some infants with a severe HPeV infection may show adverse neurodevelopment, and follow-up by a pediatrician is recommended[8-10]. Hyper-cytokinemia is suspected as the biochemical background of HPeV infections[11,12]. We experienced several infantile cases of HPeV infection and assessed their interleukin-6 levels.
A 2-month-old boy visited a clinic due to high fever and poor feeding. He was previously healthy with no family history of infection. Sepsis was suspected, and he was transferred from the clinic to a local hospital. After multiple cultures were done, antibiotic treatment was begun. On day 2, during a brain MRI under sedation, the patient presented apnea leading to respiratory difficulty with foamy sputum. The MRI was discontinued, and the patient was intubated immediately. A chest XP and CAT scan revealed decreased permeability of the bilateral lungs(Fig. 1(a),(b)). An echocardiogram disclosed an ejection fraction of 10%, and he was referred to our hospital for further treatment.
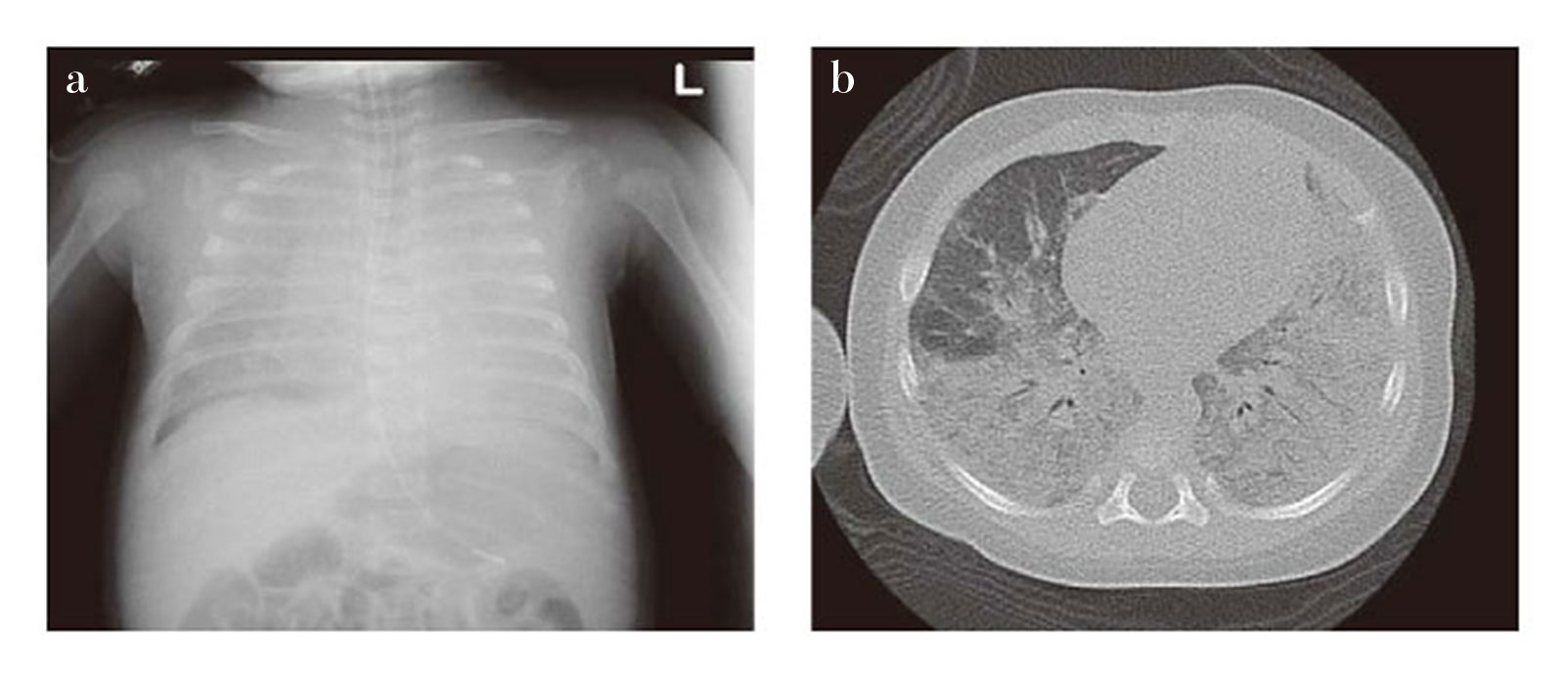
Fig. 1 Chest XP and CAT scan of this case
(a) XP
(b) CAT scan
On admission to the pediatric ICU his vital signs showed tachycardia (HR over 180’s/minute) and hypotension(systolic BP under 60’s mmHg) while the blood gas analysis showed a high lactate level(over 5 mmol/dL). His clinical condition put him at risk of cardiogenic shock. Inotrope and lucinotrope(epinephrine and milrinon) were started. The spectrum of the antibiotics was broadened, and a high dose of corticosteroid for sepsis was administered. During the course of his ICU stay, he required intermittent use of high frequency oscillatory ventilation(HFOV) but was extubated on ICU day 9 and discharged from the ICU on day 10(Fig. 2).
The serum interleukin-6(IL-6) level was measured in this case(ICU day 1) by RAY-FASTTM(TORAY Co., Ltd), however, IL-6 was not elevated.
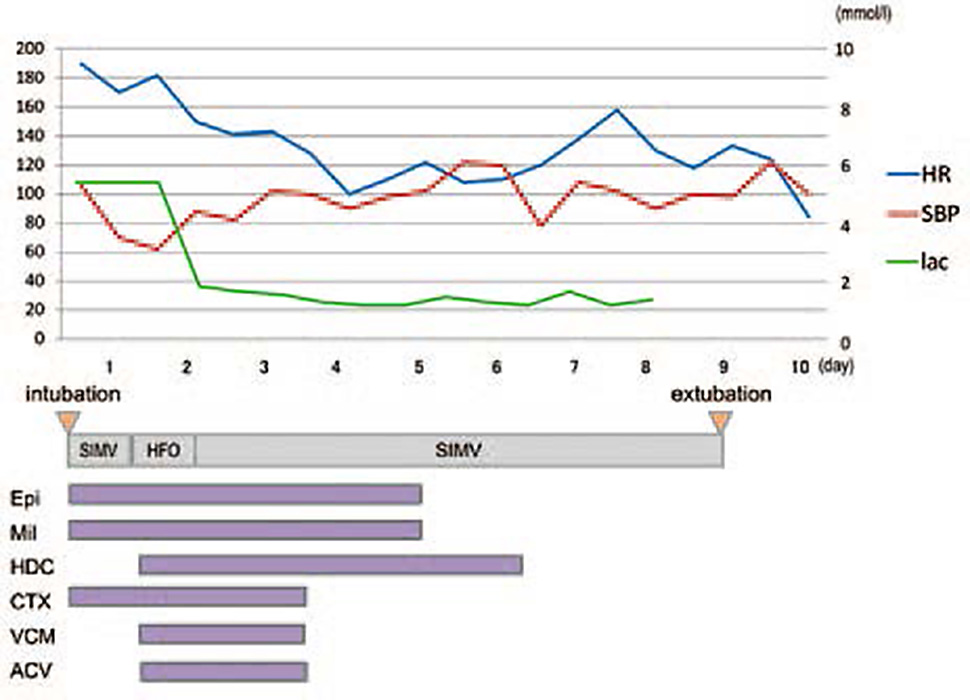
Fig. 2 Clinical course of this case in the pediatric ICU
HPeV is increasingly being recognized as a potentially severe viral infection in infants. HPeV belongs to the family Picornaviridae and is currently divided into 19 genotypes[13]. HPeV-1 is the most prevalent genotype and commonly causes gastrointestinal and respiratory disease. HPeV-3 is clinically the most important genotype due to its association with severe disease states in younger infants, which may partly be explained by its distinct virological properties [14-16]. In young infants, the typical clinical presentation includes fever, irritability, and rash, which account for the description of the patients as“ hot, red, angry babies”[1].
Although HPeV infection increases the risk of long-term neurological sequelae, the clinical course is self-limiting even when ICU admission is required. Molecular diagnosis for early detection should be included in the standard assessment for sepsis-like illnesses and general supportive critical care[17]. Early diagnosis is helpful for minimizing the unnecessary use of broad spectrum antibiotics, predicting the clinical course in the ICU, and preparing long-term, postdischarge neurological follow up.
Several studies suggested that the serum and/or cerebrospinal fluid(CSF) cytokine levels change in HPeV infections. While Fortuna reported that CSF IL-6 and IL-8 were not elevated in HPeV cases[11], Yokota demonstrated that serum IL-6, IL-10, and interferon gamma were elevated in severe cases[[12]. Fortuna measured cytokines levels comparing HPeV and enterovirus(EV), and he concluded that the immune response to HPeV infection differs from that of EV. Yokota measured cytokine levels in HPeV type 3 only. HPeV was known to have several genotypes[17], and type 3 is also known to be severe and show sepsis like clinical picture[5,6]. Our case showed no elevation of IL-6 on ICU day 1, however, we didn’t analyze genotypes and this is one of our report limitations. The immune response in HPeV infections is not yet fully understood, and further research is needed for clarification.
NS, EM, TK, and OS managed the case. TK measured IL-6. NS, EM, TK, and OS contributed to writing of the report. Consent to publication was obtained from the family. Publication was approved by the Institutional Review Board of Tokyo Metropolitan Children’s Medical Center. Authors thank Mr. James Robert Valera for his assistance with editing the manuscript.
Address correspondence to Dr. Naoki Shimizu.
Department of Pediatric Emergency & Critical Care Medicine, Tokyo Metropolitan Children’s Medical Center, 2-8-29, Musashidai, Fuchu, Tokyo 183-8561, Japan.
Phone: +81-42-300-5111. Fax: +81-42-312-8160.
E-mail: naoki_shimizu@mac.com
