




Volume 83, Number 4
[Case Report]
Eriko Yahata, Hideo Yoshida, Tadashi Matsunaga, Katsunori Kouchi
Hiroaki Kuroda, Tomoro Hishiki, Takeshi Saito, Shin-ichi Yamada
Keita Terui and Naomi Ohnuma
(Received February 14, 2007, Accepted April 4, 2007)
Surgical management of gastroschisis associated with intestinal atresia is often difficult. We successfully treated two such gastroschisis cases, including one with an intestinal perforation. In both cases, primary repair of the intestinal atresia was not possible because of intestinal edema. The first case had jejunal atresia. We performed a staged repair of the abdominal wall using a silo and decompressed the gastrointestinal tract via a nasogastric tube. The second case had colonic atresia and the caecum was perforated. We constructed a silo pouch and inserted a drainage tube into the intestine through the perforation site. In the first case, the silo was progressively tightened and the intestine was repositioned into the abdominal cavity in six days, and a delayed anastomosis was safely performed at nine days of age. In the second case, we performed an abdominal wall closure and stoma construction five days after birth. Stoma closure was performed at 70 days of age. In both cases, the postoperative course was uneventful. Intestinal atresia in gastroschisis cases can be safely managed with a delayed repair. In these cases, a nasogastric tube was adequate for decompression; and tube drainage via the perforation site may be recommended in those with intestinal perforation.
Gastroschisis, Intestinal atresia, Intestinal perforation, Silo
Intestinal atresia occurs in approximately 10% to 20% of patients with gastroschisis [1] . Treatment of such cases is often difficult and the association of intestinal atresia is reported to increase the mortality of gastroschisis cases [1-3] . However, the optimum surgical management still remains a matter of debate. We herein describe the successful treatment of two such gastroschisis cases, including one accompanied by an intestinal perforation.
Gastroschisis with intestinal atresia was diagnosed by ultrasound at 30 weeks of gestation in a female fetus; the infant was delivered vaginally at 37 weeks of gestation, and weighed 2434 grams. Severe intestinal edema and adhesion prohibited primary abdominal wall closure and she underwent silo repair two hours after birth. At that time, the intestinal atresia site could not be ascertained. Radical abdominal wall closure and delayed primary intestinal anastomosis was performed nine days after birth. At the second surgery, the intestinal edema had decreased and the adhesions were dissolved; the procedure for the combined abnormality progressed well without difficulty. Prior to this radical procedure, only a nasogastric tube was necessary for decompression. The patient did well postoperatively and was discharged at 85 days of age.
A 2502-gram female infant was delivered vaginally at 36 weeks of gestation; no anomalies had been noted during the prenatal course. At birth, gastroschisis with an intestinal perforation was found. Seven hours after birth, the first operation was performed. At that time, the intestinal abnormality, which caused perforation, could not be ascertained because of the intestinal edema and adhesions. Therefore, we decided to perform a staged repair. The first operation included a silo repair for the abdominal wall defect, and a tube drainage, which was inserted into the intestine via the perforation site. Additional soft tubes were placed inside of the silo pouch to drain overflowed intestinal contents (Fig. 1, 2). Five days after birth, a second operation was performed. At surgery, the intestinal edema and adhesion was improved and intestinal atresia was suspected as the cause of the perforation; however, the specific atretic site was not apparent. We performed a closure of the abdominal wall defect and made an enterostomy at the perforation site. A barium enema at 63 days after birth revealed a microcolon. At 70 days of age, a third operation was performed. At surgery, the colonic atresia was confirmed and the perforation site was found at the caecum; an intestinal anastomosis was made. The patient did well postoperatively and was discharged 35 days after the last operation (105 days of age).

Fig. 1
Case 2; First operation. A drainage tube was inserted into the intestine through the perforation site (white arrow head). A silo was applied thereafter.
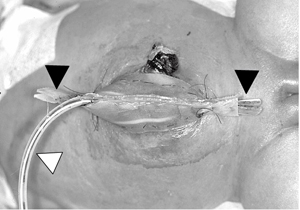
Fig. 2
Case 2; Four days after the first operation. The prolapsed intestine is almost repositioned into the abdominal cavity. The white arrowhead indicates the drainage tube inserted into the intestine through the perforation site. The black arrow head indicates the soft tubes that were placed inside of the silo to drain the overflowed intestinal contents.
Currently, gastroschisis is recognized as a disease with a good prognosis and the mortality rate has been reported to be 0 to 8 % [1,2,4,5] . However, if the condition is complicated by intestinal atresia, its management and treatment becomes more difficult. Several investigators have identified intestinal atresia as a marker for increased mortality in gastroschisis [1-3] . Furthermore, intestinal perforation, which makes the situation even more complicated, occurs in 12.5 to 20 % of gastroschisis cases with intestinal atresia [2,3,6] . In Japan, 36 cases of gastroschisis, accompanied with intestinal atresia, have been reported, and seven cases (13.9 %) were complicated with an intestinal perforation. Strategies for these conditions are not yet established, and it still remains controversial about the timing of intestinal anastomosis and the indication of enterostomies.
Case 1 had an intestinal atresia at the jejunum, which had been diagnosed prenataly. At birth, the thickened and edematous intestine contraindicated the performance of a primary anastomosis. Therefore, we chose a delayed primary anastomosis, using a nasogastric tube for intestinal decompression. Prior reports have suggested that if the intestine is of good quality with an isolated atresia and limited proximal dilation, primary anastomosis can be selected. If excessive intestinal adhesion and edema (peel) prohibits a primary anastomosis, delayed primary anastomosis is preferred than enterostomy, since stomas might lead to major complications [1-3,6,7] . The advantage of delayed primary anastomosis is that the bowel softens rapidly within 7 to 14 days once returned to the abdominal cavity, making the anastomosis much easier [2] . In our case, we could not perform primary abdominal closure and a silo was placed initially. Nine days later, the intestinal peel was improved markedly and we were able to perform a delayed primary anastomosis. However, only in cases in which the proximal intestine is grossly dilated, enterostomy must be considered to allow maximal deflation of the proximal intestine [3] .
Case 2 had ascending colonic atresia with a caecal perforation. Excessive intestinal peel made it impossible to perform both a primary abdominal closure and an enterostomy; therefore, a silo repair was required. It is generally considered that in perforated cases, stoma construction is required for safe management [2] . However, stoma construction is recommended to take place at the time of abdominal closure, [1] since the combination of silos and stomas makes the management complicated and increases the risk of infections. Therefore, in perforated cases that require silo repair, it is necessary to avoid the leakage of intestinal content from the perforation site until abdominal wall closure and stoma construction becomes possible. Oversewing the perforation site may be one strategy for this condition [2] . We considered that oversewing an edematous, thickened, and dilated intestine might carry a risk of re-perforation. As an alternative strategy for local control of the perforation site, we inserted a drainage tube into the intestine via the perforation site and successfully drained the intestinal content. As a result, the intestinal peel was lessened and safe stoma construction could be performed at the second surgery. We recommend this strategy in perforated cases that require a staged abdominal closure.
腸閉鎖を合併した腹壁破裂の治療にはしばしば難渋する。我々は腸閉鎖を合併した腹壁破裂2例を経験し,効果的な治療を行うことが出来たので報告する。出生時,2例とも脱出腸管が多く,腸管の浮腫が著明であったことから,一期的腹壁閉鎖は不可能であった。腸閉鎖に対しては,浮腫著明な腸管を一期的に切除吻合することは出来ず,また人工肛門造設も出来ない状況であった。症例1は空腸閉鎖を合併していた。まずは腹壁破裂に対して,サイロを用いた多段階腹壁閉鎖術を選択した。同時に空腸閉鎖に対しては経鼻胃管チューブを用いて口側腸管の減圧を図った。サイロを徐々に縫縮し,日齢6に脱出腸管を全て腹腔内に還納することが出来た。そして日齢9に,空腸閉鎖に対する根治術を問題なく施行することが出来た。症例2は結腸閉鎖と,盲腸穿孔を合併していた。症例2でも腹壁破裂に対して,まずサイロを造設した。結腸閉鎖・盲腸穿孔に対しては,穿孔部にドレーナージチューブを挿入して減圧した。症例1と同様にサイロを徐々に縫縮し,日齢5に脱出腸管を全て腹腔内に還納できた。この時,同時に人工肛門を造設し,穿孔部が人工肛門となるようにした。人工肛門閉鎖・腸閉鎖根治術は完全に腸管の浮腫が改善する時期を待って,日齢70で施行した。症例1,2ともに最終手術後の経過は良好である。腸閉鎖を合併した腹壁破裂に対して,いずれも待機的な腸閉鎖根治手術が有効であった。症例1では,根治手術までの間の経鼻胃管チューブが口側腸管の減圧に有効であり,症例2では穿孔部に挿入したドレーナージチューブが,減圧と感染予防の点で有用であった。
Department of Pediatric Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
八幡江里子,吉田英生,松永正訓,幸地克憲,黒田浩明,菱木知郎,齋藤 武,山田慎一,照井慶太,大沼直躬: 腸閉鎖を合併した腹壁破裂の2治験例.
千葉大学大学院医学研究院小児外科学
Tel. 043-222-7171. Fax. 043-226-2366.
2007年2月14日受付,2007年4月4日受理.
