




Volume 83, Number 5
[Case Report]
Katsuhiro Hanawa1), Toshiyuki Oshitari1),
Hiroshi Nagata2) and Emiko Adachi-Usami1)
(Received April 3, 2007, Accepted April 13, 2007)
We report 6 patients with binasal visual field defects; two had been followed as cases of primary open angle glaucoma, one with normal tension glaucoma, and three with ocular ischemic syndrome. The 6 patients underwent magnetic resonance imaging to rule out neurological disorders, and all cases were found to have an empty sella turcica or the empty sella syndrome. In all of the 6 cases, there was no progression of the visual field defects during the period of this study. Thus, the empty sella syndrome and optic neuropathy possibly caused by carotid artery stenosis should be considered before a diagnosis of glaucoma is made in cases with glaucoma-like visual field defects to prevent unnecessary glaucoma treatment.
empty sella, normal tension glaucoma, magnetic resonance imaging, binasal visual field defects, visual evoked cortical potential
The Tajimi Study reported that 90% of the open angle glaucoma patients in Japan have normal tension glaucoma (NTG)[1], and the therapy recommended for these cases was to lower the intraocular pressure (IOP) to levels lower than the “normal pressure”. However, the glaucomatous visual field changes can progress even with lower IOPs. Therefore, it is very important to rule out other diseases such as the optic neuropathies, e.g., ocular ischemic syndrome (OIS) or intracranial diseases, before a definitive diagnosis of NTG is made. Among these neurological diseases, those affecting the optic nerve or chiasma should always be considered because they can produce visual fields defects that can resemble glaucomatous visual field defects.
The empty sella (ES) syndrome is one of the neurological diseases which is associated with visual field defects that can be interpreted as being due to glaucoma [2-5]. A definitive diagnosis of ES syndrome can be made by skull X-rays, by computed tomographic (CT) scans especially with the metrizamide CT scans, and presently by magnetic resonance imaging (MRI)[2-6]. After the Tajimi Study, however, there has not been any report stressing the importance of ruling out the ES syndrome before a diagnosis of glaucoma including NTG is made.
We report 6 cases with binasal visual field defects that were treated as either glaucoma or OIS. However, MRI showed that all had the ES syndrome.
Fourteen patients who have had binasal visual field defects without a nerve fiber layer defect (NFLD) since 2003 underwent MRI to rule out orbital and intracranial lesions as the cause of the visual defect. Coronal, sagittal and/or horizontal sections of T1, T2, and Gadonium-enhanced images were recorded. The maximum rod and cone electroretinograms (ERGs) and pattern visually evoked cortical potentials (VECPs) were also recorded, if necessary.
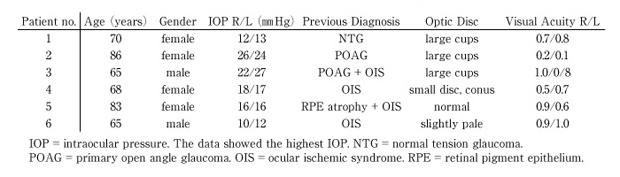
The procedures used followed our institutional guideline, and conformed to the tenets of the World Medical Association Declaration of Helsinki. An informed consent was obtained from all participants. The demographic data of all six patients are shown in table 1.
Table 1
Clinical data of six patients with binasal visual field defects and empty sella.
Among 14 patients, 8 cases showed no ES and they have been followed up as primary open angle glaucoma (POAG) or NTG. We described here 6 cases with ES.
A 70-year-old woman was referred to us by a neighboring ophthalmologist as possibly having NTG. Her visual acuities were 0.7 OD and 0.8 OS, and her IOPs were 12 mmHg OD and 13 mmHg OS. The cup/disc (C/D) ratios were 0.7 OD and 0.9 OS with undermining of the temporal vessels and a thin rim. No NFLD was found in both eyes. Humphrey perimetry detected binasal visual field defects (Fig. 1). A diagnosis of NTG was made and latanoprost was prescribed.
A brain MRI was performed to rule out intracranial diseases a month later, and an ES was found in the MRI (Fig. 2) She was diagnosed as having NTG with the ES syndrome, and was followed without any medications. Her IOPs have been kept at 9 mmHg OD and 8 mmHg OS, and the visual field defects did not change for 3 years.
An 86-year-old woman visited our hospital complaining of blurred vision in both eyes. Her visual acuities were 0.2 OD and 0.1 OS with relatively severe nucleo-cortical opacities of the lens in both eyes. Her IOPs were 26 mm Hg OD and 24 mmHg OS. Phacoemulsification with intraocular lens implantation was performed on the right eye, and vision improved to 1.2. She refused cataract surgery on her left eye. Goldmann perimetry showed binasal visual field defects (Fig. 1), and timolol maleate was prescribed because the IOPs remained high. Fundus examination showed large cups and pale discs with C/D ratios of 0.7 in both eyes, and we added unoprostone. No NFLD was found.
To confirm the diagnosis of glaucoma, MRI was done and an ES was found (Fig. 2). She was diagnosed with cataract and POAG with the ES syndrome. The binasal visual field defects have been unchanged during the one year follow-up period but this period was too short to determine definitively which disease caused the binasal visual field defects.
A 65-year-old man visited our clinic complaining of blurred vision in both eyes. His visual acuities were 1.0 OD and 0.8 OS, and the IOPs were 22 mmHg OD and 27 mmHg OS. Ophthalmoscopy revealed very narrows arteries, large C/D ratios, and pale optic discs in both eyes. The disc of the right eye showed a notch at the inferotemporal margin but no NFLD. Humphrey perimetry demonstrated binasal visual field defects in both eyes (Fig. 1). The implicit time of the P100 component of the pattern VECPs was significantly delayed in both eyes and ultrasound Doppler examination of the cervical arteries showed a stenosis of both common carotid arteries. Fluorescein angiography demonstrated delayed arm-to-retina time. A diagnosis of POAG accompanied by OIS was made. To rule out intracranial diseases, MRI was performed and an ES was found. He was diagnosed with POAG and OIS with the ES syndrome.
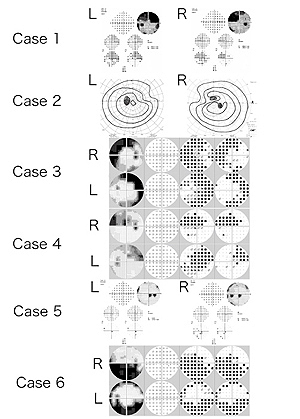
Fig. 1
Humphrey and Goldmann perimetric findings in all cases. The Humphrey and Goldmann perimetric findings show visual fields resembling glaucomatous defects in both eyes of all cases. In Cases 3, 4, and 6, the figures are shown as grey scale images. The findings of the threshold tests, total deviations, and pattern deviations are shown on the left.
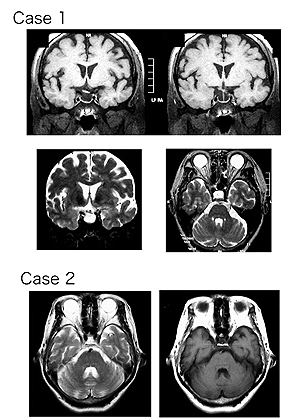
Fig. 2
MR Images of the brain of Cases 1 and 2. Note the empty enlarged sella turcica and tilted chiasma in Case 1. The upper figures are T1 and the lower figures are T2 images in Case 1. The left figure is T2 and the right figure is T1 image in Case 2.
A 68-year-old woman reported a transient visual loss of several seconds. Her visual acuities were 0.5 OD and 0.7 OS. Nuclear cataracts were found in both eyes. Fundus examination showed a slightly smaller disc with a large conus and inferior sectorial choroidal atrophy in her right eye. Her IOPs were 18 mmHg OD and 17 mmHg OS. Humphrey perimetry showed binasal visual field defects (Fig. 1). The retinal arteries in both eyes were extremely narrow with bright reflexes. The implicit time of the P100 of VECPs was significantly delayed but the maximal rod and cone ERGs were normal in both eyes. An ultrasound Doppler examination of the cervical arteries showed reduced blood flow in both common carotid arteries. A possible diagnosis of OIS was made. MRI was performed and an ES was found. She was diagnosed with possible OIS with the ES syndrome.
An 83-year-old woman had undergone phacoemulsification and intraocular lens implantation in both eyes. Although her vision improved to 0.9 OD and 0.6 OS, Humphrey visual field showed binasal inferior scotoma encroaching on the central field (Fig. 1). Ophthalmoscopy revealed multiple drusen with normal discs in both eyes. Fluorescein angiography revealed hyperfluorescence corresponding with the drusen and retinal pigment epithelial atrophy in the macular region of both eyes. The maximal rod and cone ERGs were normal in both eyes, and the implicit time of P100 of VECPs was delayed in the right eye and non-recordable in the left. MRI demonstrated an ES. An ultrasound Doppler examination of the both cervical arteries showed reduced blood flow. She was diagnosed with retinal drusen and retinal pigment epithelium atrophy and possible OIS accompanied by the ES syndrome. For the past 3.5 years, her visual field and visual acuities have remained unchanged.
A 65-year-old man had undergone surgery to remove a meningioma of the frontal lobe region 25 years earlier. He visited our clinic complaining of photopsia of several days duration. His visual acuities were 0.9 OD and 1.0 OS, and both optic discs were slightly pale without glaucomatous excavation. The retinal vessels were narrow. Humphrey visual fields showed binasal inferior hemifield defects (Fig. 1). An ultrasound Doppler examination showed sclerotic changes of both common carotid arteries. The implicit time of P100 of VECPs was slightly delayed in both eyes. MRI showed an ES. We have been following him with a tentative diagnosis of OIS accompanied by the ES syndrome, and his visual field defects have remained unchanged for 2.5 years.
The ES syndrome is an anatomical condition in which the pituitary tissue is flattened against the subarachnoid membrane that has dropped into the sella turcica [7]. Patients with the ES syndrome have visual field defects which often resemble glaucomatous field defects, and the cups of the optic discs are enlarged as in glaucomatous eyes. The visual field defects are probably induced by negative pressure on the optic nerve or chiasma [7].
In Cases 1-3, we could not determine definitively whether a glaucomatous optic neuropathy coexisted with the ES syndrome. However, Case 1 was being treated as a case of NTG and after the anti-glaucoma therapies were stopped, the visual field defects did not progress. Case 2 and 3 have been treated as POAG and followed up 1 to 4 years since the ES was found and the field defects remained unchanged. These findings suggest that the ES syndrome was most likely the cause to the binasal field defects. These patients are being followed to verify that the cause of the visual field defects is the ES syndrome.
It is very important to rule out other diseases in cases of NTG, however, we are not aware of any report that has stated the importance of ruling out the ES syndrome in patients with NTG. Before the Tajimi Study, there were some reports on the existence of the ES syndrome in some patients being followed as NTG patients [2-5]. In these reports, most patients with the ES syndrome had binasal field defects, but only a few studies used MRI examinations to verify the ES syndrome. Because of the importance of ruling out intracranial diseases to make a definitive diagnosis of NTG, MRI is recommended because it is less invasive than any other examination methods.
In Japan, the incidence of glaucoma is 5.0% of the general population over 40-years-of-age. On the other hand, ES may occur at a higher incidence than glaucoma according to a biopsy study of the sella turcica [8]. Therefore, the ES syndrome is the most important neuronal disorder to rule out before a diagnosis of NTG is made.
VECPs were recorded from four patients (Case 3-6) to rule out ischemic optic neuropathies. In all cases, the implicit time of the P100 of VECPs was delayed. In the end, the abnormal VECP findings directed us to perform ultrasound Doppler examinations that led to the find common carotid artery stenosis and MRI to find the ES syndrome.
OIS, including ischemic optic neuropathy, is one of the neuronal disorders in which binasal visual field defects resembling glaucomatous optic neuropathy is found. Thus, it is very important to rule out ES syndrome before making a diagnosis of glaucoma or OIS. In addition, the results of VECPs suggested the usefulness of VECPs together with Doppler echography in identifying OIS accompanying with intracranial diseases including common carotid artery stenosis and ES.
In conclusion, we report 6 patients with binasal field defects who were diagnosed with glaucoma and/or OIS but found to have the ES syndrome from the MRI findings. Thus, before a diagnosis of glaucoma including NTG or OIS is made, ophthalmologists should carefully rule out the ES syndrome as the cause of the glaucomatous visual field defects.
We thank Professor Duco Hamasaki for helpful edit works.
両鼻側視野障害を呈した6例のEmpty Sella症候群を報告する。2例は原発開放隅角緑内障, 1例は正常眼圧緑内障, 3例は眼虚血症候群として経過を見ていた症例である。頭蓋内疾患を除外するためMRIを施行したところ全例にEmpty Sellaが観察された。6例ともに経過観察中に視野の進行は確認されなかった。不必要な緑内障治療を避けるためにも, 両鼻側視野異常のような緑内障様の視野異常を呈した症例においては緑内障の診断を下す前にEmpty Sella症候群や頚動脈狭窄症に起因する視神経症の可能性を考慮することが重要である。
1) Department of Ophthalmology and 2) Department of Oto-Rhino-Laryngology, Center for Sensory Organ Diseases, Sannoh Medical Center, Chiba 263-0002.
塙 勝博1), 忍足俊幸1), 永田博史2), 安達惠美子1): 両鼻側視野障害を呈したEmpty Sella症候群の6例.
1) 山王病院感覚器病センター眼科, 2) 耳鼻咽喉科
Tel. 043-421-2221. Fax. 043-421-3072. e-mail: Tarii@aol.com
2007年4月3日受付, 2007年4月13日受理.
