




Volume 83, Number 6
[Original Paper]
Masako Mizoguchi1), Yutaka Momota1), Takashi Kobayashi1)
Hiroyuki Matsue1), Hiroshi Shinkai1) and Atsushi Utani2)
(Received June 4, 2007, Accepted July 2, 2007)
Prognosis of vascular Ehlers-Danlos syndrome (EDS) is very poor because of rupture of arteries, the intestine or uterus. Early diagnosis is desirable but it is difficult to diagnose as skin hyperextensibility and joint hypermobility are generally mild. For a definitive diagnosis, detection of reduced secretion of type III collagen or identification of COL3A1 mutations by DNA sequencing needs to be performed. Although reduced type III collagen secretion has been detected by autofluorography using radioisotopes such as 3H-proline, radioactive waste is produced and it is a time- and cost-consuming method. Here, we have established a new method for screening vascular EDS patients utilizing Western blotting. Fibroblasts were cultured from biopsied skin samples of 23 patients who had suspected vascular or classical EDS from their clinical manifestations. Type III collagen secretion in conditioned medium was reduced in 14 of 23 patients (60.9%). When vascular EDS is suspected clinically, Western blotting to assess type III collagen secretion should be considered as a first-line screening method, because it is quicker and less expensive than autofluorography or DNA sequencing.
vascular Ehlers-Danlos syndrome, fibroblasts, Western blotting
Ehlers-Danlos syndrome (EDS) is a disease characterized by skin hyperextensibility, joint hypermobility, and skin/vascular fragility caused by abnormalities of extracellular matrix components and molecules, such as collagen, associated components, or modifying enzymes. EDS is classified using a new system proposed by Beighton et al [1]. EDS types I and II are equivalent to classical EDS, caused by abnormalities in the COL5A1 or COL5A2 genes [2]. EDS types III and VI are equivalent to hypermobility type and kyphoscoliosis type EDS, respectively. Since only single cases of types V and X EDS have been reported, these types have been reclassified and incorporated into the other types according to this new system [1]. EDS type VII is classified into two types, arthrochalasia and dermatosparaxis type EDS.
EDS type IV is equivalent to vascular EDS and it often causes a fatal rupture of an artery, intestine or uterus [1]. Vascular EDS is an autosomal dominant disorder and caused by a mutation in the COL3A1 gene, which spans 44 kb with 52 exons [1]. While thin skin, translucent vessels, vascular fragility, propensity to internal bleeding and hypermobility of small joints are seen, these features are often mild. In many cases, vascular EDS patients die in their 30 and 40s due to sudden arterial rupture. Because vascular EDS has the poorest prognosis in all EDS types [1, 3], early diagnosis is desirable. However, according to past reports, there are few common COL3A1 mutations observed in patients and the relationship between the type of mutation and clinical symptoms has not been clarified [4-7]. A test for COL3A1 mutations needs to be performed on the entire COL3A1 gene, but this is a time- and cost-consuming approach because of the large size of the gene and the multiple number of exons. Hence, there is a need to establish a screening method that can conveniently and rapidly reach a diagnostic conclusion.
Because type III collagen is a homotrimer consistng of three identical polypeptide chains, written as [α1 (III) ] 3, a mutation of a single allele can reduce secretion of normal type III collagen molecules to one eighth ( (1/2) 3)[7]. Each of the remaining seven eighths molecules including an abnormal α1 (III) chain are rarely secreted and those molecules that are secreted are nonfunctioning and are quickly degraded. This distinctive decrease of secreted type III collagen is therefore a valuable tool to screen for vascular EDS. Until now, reduced secretion of type III collagen in vascular EDS has been detected by autofluorography.
In order to establish a simple method to conveniently detect reduced secretion of type III collagen, specific monoclonal antibodies and Western blotting was utilized. Dermal fibroblasts were grown from skin biopsies collected from 23 patients who were suspected as having classical or vascular EDS. The amount of type III collagen secreted by fibroblasts into the medium was analyzed by Western blotting. This represents a unique method for screening vascular EDS without the use of radioactivity.
Fibroblasts were prepared from the outgrowth of dermal tissue obtained from skin biopsies of 23 patients with suspected classical or vascular EDS after obtaining their informed consent. For comparison, fibroblasts were also grown from skin biopsies of eight healthy individuals. Fibroblasts were maintained in Dulbecco’s modified Eagle’s medium (DMEM) supplemented with antibiotics and 10% fetal calf serum (FCS). Fibroblasts within 3-6 passages were used for this study. Fibroblasts were seeded in 35-mm dishes and were cultured at 37℃ under 5% CO2 until nearly confluent. This was followed by incubating with 10%FCS/DMEM containing 50μg/ml ascorbic acid for an additional 24 hours. Fibroblasts were washed twice with 2 ml of phosphate-buffered saline (PBS) and incubated in 2 ml of CD CHO medium (Invitrogen, Carlsbad, CA, USA) supplemented with L-glutamine and antibiotics. After a further 48 hours, conditioned media was collected and dialyzed against distilled water for 48 hours at 4 ℃.
Dialyzed conditioned media were lyophilized and dissolved in 60 μl of SDS-PAGE sample buffer. Fifteen μl samples were boiled for 7 minutes at 104℃ in the presence of 2% mercaptoethanol. Proteins of each sample were electrophoresed on 6% SDS polyacrylamide gels and transferred to Immobilon-P Transfer Membranes (Filter type: PVDF, pore size: 0.42 mm, Millipore, Bilerica, MA, USA). Each membrane was preincubated with blocking buffer (TBST with 5% nonfat milk) for 30 minutes at room temperature. Anti-human type III collagen monoclonal antibody (Daiichi Fine Chemical Co., Ltd., Toyama, Japan), an antibody made against total α1 (III), was diluted at 1:400 in 5% milk/TBST and was incubated overnight at 4℃. The membrane was washed three times with TBST for 5 minutes each. Horseradish peroxidase-conjugated anti-mouse IgG antibody (Amersham Biosciences, Buckinghamshire, UK), diluted 1:2000 in TBST, was incubated at room temperature for one hour, followed by washing three times for 5 minutes each in TBST. The ECL Western blotting detection reagents and analysis system (Amersham Biosciences) were used and the membrane was exposed to Hyperfilm (Amersham Biosciences).
To confirm that similar amounts were loaded on the blotting membrane, type I collagen was probed as an internal control, after stripping the type III collagen antibodies with heated buffer, as described in the ECL protocol (Amersham Biosciences). Anti-human type I collagen (C-18) antibody (sc-8786, Santa Cruz Biotechnology, Inc., Santa Cruz, CA, USA), the epitope of which is localized at the carboxy terminus of the α2 (I) chain, was diluted in TBST at 1:240 and incubated with the membrane overnight at 4℃. The membrane was washed three times using TBST for 5 minutes each, and then was incubated with peroxidase-conjugated AffiniPure F (ab’) 2 fragment donkey anti-goat IgG (H+L) (Jackson ImmunoResearch Laboratories Inc., West Grove, PA, USA; dilution 1:3000) for one hour at room temperature. The membrane was again treated with the ECL Western blotting detection reagents and analysis system as above. In some cases, type I collagen was also detected using alkaline phosphatase-conjugated AffiniPure donkey anti-Goat IgG (H+L) (Jackson ImmunoResearch Laboratories Inc., ; dilution 1:2000) as a secondary antibody, followed by visualization with alkaline phosphatase substrates (Moss Inc., Pasadena, MD, USA).
Table 1 summarizes the clinical features and the amount of type III collagen secretion of the 23 patients on whom Western blotting was performed. Of the 23 patients screened, clinical findings suggested vascular EDS in 14 patients. These clinical findings included a family history of vascular EDS, or symptoms suggestive of vascular EDS in patients younger than 50 years of age, such as cardiovascular abnormalities, sudden death, pneumothorax, and/or pulmonary bleeding. The remaining nine patients did not exhibit any of these symptoms or have a family history of vascular EDS. Four cases with decreased type III collagen secretion and with different clinical features are presented below:
Table 1
Clinical features of 23 Japanese patients and results of Western blotting
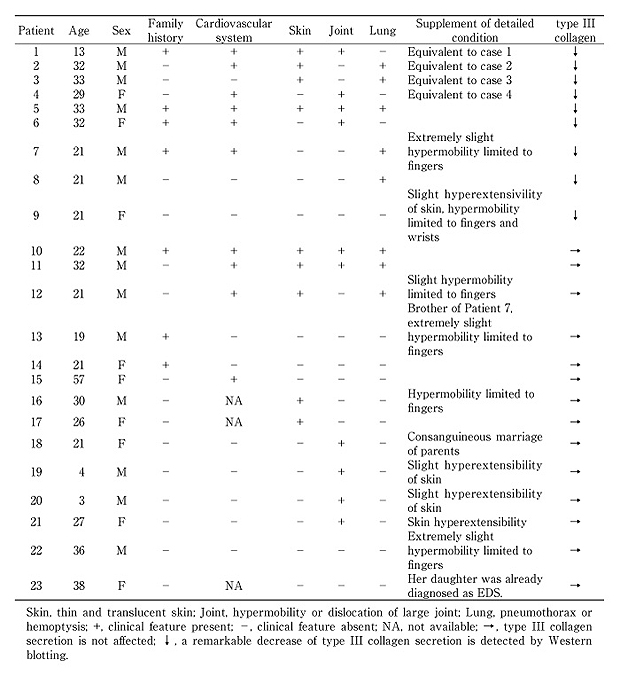
A 13-year-old boy presented with skin hyperextensibility and joint hypermobility of the fingers and elbow since infancy. Habitual dislocations of the shoulder joint and valvular abnormalities were detected in his childhood. His father died due to a ruptured aneurysm at age 40 years. His older brother died suddenly during a physical education class at the age of 17 years. Physical examination revealed skin hyperextensibility and joint hypermobility of the elbows, hands, feet, fingers, and toes (Fig. 1). There were no notable problems with the lungs, digestive tract or eyes, and hematological tests showed no abnormalities in blood count, bleeding time, or coagulation. Fig. 2 shows histological sections of his skin. Under low magnification, dermal collagen fibers appeared rough and aberrant. Under high magnification, the thickness of the collagen fibers was uneven and ruptured fibers were seen. These histological changes of the skin were also observed with Cases 2 through 4.
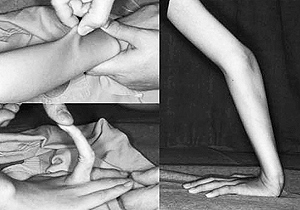
Fig. 1
Clinical appearance of case 1. Hyperextensi-bility of antebrachial skin was confirmed, while examination of the joints revealed hypermobility of the elbows and fingers.
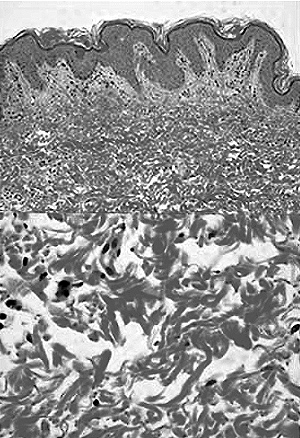
Fig. 2
Histological skin sections of case 1. Under low magnification, dermal collagen fibers appeared rough and aberrant. Under high magnification, the thickness of collagen fibers was uneven and ruptured fibers were seen.
A 32-year-old man had undergone thoracic surgery for spontaneous left pneumothorax, but as it recurred four months later, the patient underwent a thoracotomy at the age of 21 years. At ages 23 and 25, the patient developed spontaneous right pneumothorax, which resolved with conservative management. At the age of 26 years, the patient developed right chest pain, spasm, and hemoptysis and he was admitted to hospital. A right thoracotomy was performed, which confirmed bulla accompanied by bleeding. At the age of 32 years, the patient had massive hemoptysis and 3 months later, the patient suddenly lost consciousness. Since vascular EDS was suspected, he was referred to our department. Physical examinations found mild skin hyperextensibility, but joint hypermobility was absent (Fig. 3). Hematological tests showed no abnormalities in blood count, bleeding time, or coagulation.
A 33-year-old man developed cough and hemoptysis over the course of one year. Since a chest CT scan confirmed a cystic lesion in the left lung, the left lower lobe was resected thoracoscopically at the age of 33 years. Thinning of the pulmonary arterial wall, lung tissue rupture, and hematoma were found. Right pneumothorax also manifested the same year. Vascular EDS was suspected and the patient was referred to our hospital. Physical examinations found that his skin was thin and blood vessels were visible (Fig. 4).
Hypermobility or dislocation of his joints was absent. Hematological tests showed normal values of blood count, bleeding time and coagulation.

Fig. 3
Clinical appearance of case 2. The skin was thin and mildly hyperextensible, but joint hypermobility was absent.
Fig. 4
Clinical appearance of case 3. Thin skin and visible lines of blood vessels were visible in the precordium.
From infancy, a 29-year-old woman experienced habitual dislocation of the shoulder joint, hypermobility of the elbow and finger joints, and arrhythmia. At the age of 28 years, the patient underwent pacemaker implantation surgery due to arrhythmia by an atrioventricular block. Vascular EDS was suspected so she was referred to our department. Physical examinations found mild skin hyperextensibility and hypermobility of the elbows, hands, and fingers (Fig. 5). As for the cardiovascular system, the patient had developed mitral valve insufficiency at the age of 20 years. Hematological tests showed no abnormalities in blood count, bleeding time, or coagulation.

Fig. 5
Clinical appearance of case 4. Skin hyperextensibility and joint hypermobility of the fingers were seen.
Conditioned medium containing secreted collagen was obtained from the patient’s cultured fibroblasts and from normal fibroblasts (N1-N4) prepared as a control. Fig. 6 summarizes the Western blotting results for cases 1 through 4. In all four cases, reduced secretion of type III collagen, but not type I collagen, was detected when compared with type III collagen levels in normal control samples.
In 8 of the 14 patients (57.1%) with suspected vascular EDS, Western blotting confirmed reduced secretion of type III collagen. Additionally, in 1 of the 9 patients (11.1%) where vascular EDS was not suspected, Western blotting confirmed reduced secretion of type III collagen. Thin or translucent skin was observed in 9 of the 23 patients and Western blotting confirmed reduced secretion of type III collagen in 4 of these 9 patients (44.4%). Hypermobility or habitual dislocation of large joints, or at least moderate joint hypermobility, was observed in 10 of the 23 patients (43.5%), and Western blotting confirmed reduced secretion of type III collagen in 4 of these 10 patients (40%).
To perform a semi-quantitative analysis, a normal control sample (N2) was serially diluted and examined by Western blotting concurrently with a sample of case 2 (Fig. 7). The amount of type III collagen of case 2 was similar to approximately 1/8 or 1/16 of that of a normal control. Therefore, Western blotting analysis was able to detect reduced secretion of type III collagen in patients with vascular EDS. Analysis of type I collagen verified that secretion of other collagen species was not impaired.
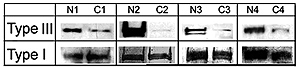
Fig. 6
Western blotting of type III collagen secretion (cases 1-4, C1-C4 and normal subjects, N1-N4). Collagens secreted into the cultured medium were probed with antibodies to α1 (III) or α2 (I). Type III collagen was remarkably reduced in patient samples, while type I collagen secretion was not affected. Column of ‘Type III’ and ‘Type I’ showed Proα1 (III) and processed Proα1 (III), and Proα2 (I) and Pcα2 (I), respectively. Proα2 (I) and Pcα2 (I) bands of C1 and C4 with its control band were detected with HRP, and Proα2 (I) and Pcα2 (I) bands of C2 and C3 with its control band were detected with ALP.
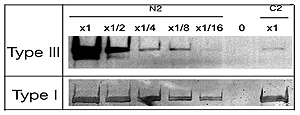
Fig. 7
Semi-quantitative demonstration of the decrease in type III collagen secretion. Samples of a normal subject (N2) were serially diluted to 1/2, 1/4, 1/8, and 1/16, followed by Western blotting with an undiluted sample of case 2. Type III collagen levels in the C2 sample were compatible to the 1/8 or 1/16 diluted N2 sample.
Vascular EDS is a rare disease with an estimated prevalence of 1:100, 000-1, 000, 000 [8], whereas the estimated prevalence of total EDS is 1:10, 000-20, 000 [3]. Vascular EDS can be difficult to diagnose based solely on clinical symptoms because joint hypermobility and skin hyperextensibility are mild. In addition, vascular EDS lacks specific histological findings. In Japan, a total of 57 cases of vascular EDS or suspected vascular EDS were reported between 1983 and 2006. In 19 patients, emergency surgery was performed and 17 of these patients had emergency surgery before vascular EDS was suspected or diagnosed. The remaining two patients had a past history of abdominal wall hematoma, intestinal membrane hematoma, and intestinal membrane artery dissection and as a result they were diagnosed with vascular EDS. Of the 57 reported cases, 19 patients (33.3%) died and only five of these 19 patients were diagnosed with, or were suspected of having, vascular EDS while alive. Thus it is difficult to diagnose vascular EDS.
Of the 23 patients in the present study, Western blotting confirmed reduced secretion of type III collagen in 9 patients (39.1%). Based on clinical findings, vascular EDS was strongly suspected in 14 of the 23 patients. In 8 of these 14 patients (57.1%), Western blotting confirmed reduced secretion of type III collagen. When vascular EDS was suspected, Western blotting confirmed reduced secretion of type III collagen in more than half. It therefore appears to be useful to screen for reduced type III collagen secretion if a patient has a family history of the disease and cardiovascular or pulmonary lesions. Western blotting confirmed reduced secretion in type III collagen in 1 of the 9 patients (11.1%) without family history, cardiovascular abnormalities or pulmonary lesions. There is little possibility of vascular EDS in those cases, but Western blotting for type III collagen secretion shows a rare possibility of vascular EDS among them.
Of the 23 patients examined, 4 (17.4%) exhibited thin or translucent skin and reduced secretion of type III collagen on Western blotting. Instead of subjective parameters such as thin or translucent skin, further investigations will be necessary to establish objective criteria, e.g., visible vascular alignment in the precordial region. Joint symptoms are generally absent or mild in vascular EDS [1]. However, among patients with hypermobility or habitual dislocation of large joints, or at least with moderate joint hypermobility, Western blotting confirmed reduced secretion of type III collagen in 4 patients (17.4%). Consequently, it will be important to consider vascular EDS even when the clinical findings are indicative of other types of EDS.
Even if Western blotting does not confirm reduced secretion of type III collagen, the type III collagen that is secreted may not be fully functional. Therefore, COL3A1 mutations cannot be completely ruled out based solely on reduced secretion. In fact, there has been a report of clinically mild vascular EDS due to haploinsufficiency of one COL3A1 allele in which no decrease in type III procollagen secretion was observed [9]. However, because most patients with vascular EDS have reduced secretion of type III collagen, DNA sequencing of the COL3A1 gene would confirm the diagnosis in patients with decreased type III collagen secretion.
Although no direct comparison of type III collagen secretion was made between autofluorography by metabolic labeling with 3H-proline and Western blotting, the results suggest that Western blotting is faster, more convenient, inexpensive, and useful screening technique for vascular EDS.
For referring patients, we would like to express our gratitude to Dr. Tetsuji Kawamura (Department of Respiratory Medicine, Himeji Medical Center; Case 2) ; Dr. Masahiro Aoshima (First Department of Internal Medicine, Kyorin University School of Medicine; Case 3) ; Dr. Eichi Kan (Department of Dermatology, Tokyo Women’s Medical University; Case 4).
血管型Ehlers-Danlos syndrome (EDS) は, 動脈の破裂などにより突然死が多く, 非常に予後が不良な病型であり, 早期の診断が望まれるが, 臨床症状が軽度のため診断が困難な場合が多い。同症が疑われる患者の線維芽細胞より分泌されたⅢ型コラーゲンの多寡をWestern blottingを用いて検出することがスクリーニングに役立てられるか検討した。
患者23例及び健常者皮膚より得た線維芽細胞を培養し, 培養上清より得た蛋白にSDS6%ポリアクリルアミドゲル電気泳動を行い, PVDF membraneに転写し, 抗ヒトコラーゲンⅢ型抗体を用いてⅢ型コラーゲンを検出, Ⅰ型コラーゲンについても同様に検出した。
臨床所見から積極的に血管型EDSを疑う症例は23例中14例あり, この14例中8例 (57.1%) において, Western blottingでIII型コラーゲンの分泌減少が認められた。また, 残りの9例中1例 (11.1%) においても減少が見られた。
Western blottingでⅢ型コラーゲンの分泌減少が明らかで無くともCOL3A1に遺伝子変異がある可能性は否定できないが, 減少が明らかな場合はCOL3A1の解析を待たずとも血管型EDSとして対処することが可能と考えられた。また, 血管型EDSを疑わせる異常がなくとも, Western blottingで減少を認める場合があり, EDSを疑う際は血管型の可能性を考慮し, Western blottingで蛋白質レベルでの検討を行うことは有用であると考えられた。
1) Department of Dermatology, Graduate School of Medicine, Chiba University, Chiba, 260-8670.
2) Department of Dermatology, Graduate School of Medicine, Kyoto University, Kyoto.
溝口雅子1), 百田 豊1), 小林孝志1), 松江弘之1), 新海 浤1), 宇谷厚志2): Western blottingを用いたIII型コラーゲン分泌減少の検出: そのvascular Ehlers-Danlos syndromeのスクリーニングにおける有用性.
1) 千葉大学大学院医学薬学府先端生命科学専攻基質代謝学
2) 京都大学大学院医学研究科皮膚科学
Tel. 043-226-2505. Fax. 043-226-2128. E-mail: mizoguti.m@fc-h.jp
2007年6月4日受付, 2007年7月2日受理.
