




Chiba Medical J. 94E:1~8,2018
doi:10.20776/S03035476-94E-1-P1
[ Original Article ]
Shigeo Hagiwara1), Junichi Nakamura1), Atsuya Watanabe2),
Shunji Kishida1), Sumihisa Orita1), Shoichiro Takao3),
Hiroshi Yoshioka4) and Seiji Ohtori1)
1) Department of Orthopaedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
2) Department of Orthopaedic Surgery, Eastern Chiba Medica Center, Togane 283-8686.
3) Department of Diagnostic Radiology, Tokushima University Graduate School, Tokushima 770-8503.
4) Department of Radiological Science, University of California, Irvine 101 City Drive South Orange, CA, USA 92868.
(Received May 30, 2017, Accepted July 12, 2017)
Objective: To determine whether or not three-dimensional(3D) isotropic Fast Spin Echo(FSE)-Cube improves the image quality of a two-dimensional(2D) FSE radial magnetic resonance imaging(MRI) protocol in diagnosis of hip labral tears.
Materials and Methods: Ten healthy volunteers were recruited as the control group. Imaging with fat-suppressed 3D FSE-Cube and 2D FSE-radial sequences was performed at 3.0 T. The relative signal intensity(SI) of each structure, relative signal contrast between structures of the hip and a qualitative analysis were analyzed for this group. Ten patients were recruited for the labral lesion group to evaluate the inter- and intra-observer reliability of each sequence.
Results: There were no significant differences in the relative SI of each structure for each sequence. The original and reformatted images of 3D FSE-Cube joint fluid to labrum were significantly higher in relative contrast than that of the 2D FSE-radial(p=0.0005, p=0.002). The 2D FSE-radial images demonstrated significantly higher scores than the 3D FSE-Cube sequence with respect to image blur and overall quality. Both the 3D FSE-Cube and the 2D FSE-radial sequences showed excellent inter- and intra-observer reliability.
Conclusion: The 3D FSE-Cube sequence with isotropic voxels has almost equal image quality of hip labral tears.
Acetabular labral tear, Magnetic resonance imaging, Hip joint, 3D MR imaging, radial MR imaging
The hip is the largest weight-bearing joint, which consists of the femoral head and the acetabulum, and it has an important role in standing and walking. The acetabular labrum is the fibrocartilage structure attached to the acetabular bone, which stabilizes the hip by increasing the effective depth of the acetabulum and contributing to the hydrostatic pressurization of the intraarticular space[1,2]. Several studies have indicated that a labral tear can be caused by developmental dysplasia of the hip(DDH), femoro-acetabular impingement (FAI) and / or previous trauma in pre-arthritic stages [3-6], and may require surgical treatment for relief from pain[7]. However, the diagnosis of labral tear can be challenging. A previous study reported a delay from the time of symptom onset to diagnosis, where several health-care providers were visited by patients prior to a definitive diagnosis. Some patients even underwent unsuccessful operative procedures prior to the diagnosis of a labral tear [8]. In the progression of hip joint degeneration in DDH, a labral lesion is thought to occur preceding radiographic findings on X-ray and it can be treated by bone preserving operations[4]. Therefore, early and accurate diagnoses of labral lesions can help improve patient outcome.
Magnetic resonance imaging(MRI) is a widely used method for the assessment of musculoskeletal disorders of the hip joint, that can involve the labrum, cartilage, joint space, capsule, compact and cancellous bone, and regional soft tissues[9]. Several sequences have been indicated for the evaluation of the acetabular labrum[10-12]; however the optimal sequence for a clinical decision is still controversial[13]. A twodimensional(2D) radial sequence was reported, which can include the whole labrum from anterior to posterior acetabulum[10]. The limitation of the 2D sequence is a relatively large slice thickness that can lead to partial volume artifacts. MR arthrography has been reported to have a higher sensitivity and specificity than MRI alone [14]; however arthrography is an invasive technique, which may limit its use as a screening examination.
Recently, three-dimensional(3D) fast spin-echo (FSE) sequences have been applied to the knee and a high contrast resolution has been reported[15,16]. FSECube(GE Healthcare) is a 3D-FSE acquisition with 2D-accelerated auto-calibrated parallel imaging and an extended echo train acquisition[17]. The advantage of a 3D-isotropic sequence is to provide high-quality multiplanar reformatting of the image data for 3D evaluation of the anatomy[16,18]. Although several studies have examined the clinical application of the 3D MRI of the hip[19,20], the diagnostic performance for 3D-FSE of the hip acetabular labrum without arthrography is still controversial.
The aim of this study is to compare 3D FSE-Cube to the 2D-radial sequence in image quality of the hip acetabular labrum.
Ten volunteers with no history of hip pain, and no abnormality or lower extremity trauma that required medical treatment, were recruited for the control group. The right hips of the control group(six men and four women; mean age 35.5 years; range, 30-35 years) were imaged for quantitative and qualitative analyses. A total of 10 patients were recruited to the labral lesion group (one man and nine women; mean age 43.2 years; range, 25-64 years) to evaluate the inter- and intra-observer reliability. Inclusion criteria for the labral lesion group consisted of 1) continual hip pain; 2) increased hip pain in flexion/internal rotation/adduction tes[21]diagnosed by an orthopedic surgeon; 3) early osteoarthritis (Kellgren-Lawrence(KL) osteoarthritis score of 1 or 2)
The research protocol for this prospective study was in compliance with the Helsinki Declaration, approved by the institutional review boards, and registered with the University Hospital Medical Information Network. Written informed consent was obtained from all study participants.
MRI was performed on a 3.0-T MRI system (Discovery MR750; GE Healthcare, Waukesha, WI, USA). A 32-channel torso coil was used to image the hip joints. The patients were asked to lie in a supine position with the hip joint in a neutral rotation.
The 3D FSE-Cube images were acquired in the sagittal plane with fat-suppressed proton density and the following parameters, repetition time(TR) / echo time(TE), 2000/25.4 msec; matrix, 288×288; field of view 26cm, section thickness, 0.9mm; and receiver bandwidth, ±125kHz, resulting in an isotropic resolution of 0.9mm, and a scan time of 7 min 25 s.
The 2D FSE-radial images were acquired with fatsuppressed proton density and the following parameters: TR / TE, 2000/11.8 msec; matrix, 384×384; field of view 20cm, 4mm slices; and receiver bandwidth, ± 62.5kHz. First, a localizer image was obtained in the transverse plane through the center of the bilateral femoral heads. Using this transverse localizer image, the orientation of the sagittal oblique sections through the anterior and posterior edges of the acetabulum, parallel to the acetabular opening, was determined. Radially sectioned images passing through the center of the femoral head every 30 degrees from 90 degrees anterior to 90 degrees posterior were obtained to provide oblique sagittal images(Fig.1), and the scan time was 6 min 28 s.
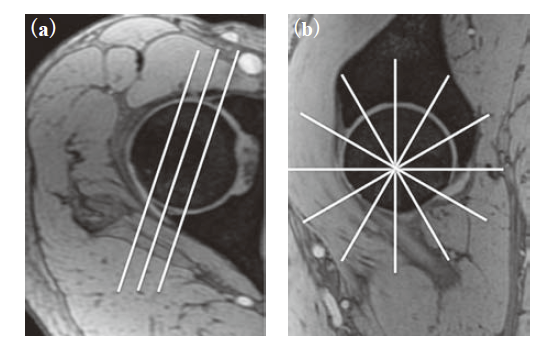
Fig. 1
(a) Transverse image through the center of femoral head. The lines indicate oblique sagittal sections through the acetabular anterior and posterior margins.
(b) Oblique sagittal image on the line of the center of femoral head. The lines indicate the direction of radialsequence images at every 30 degrees on the localizer image.
For the quantitative analysis, we measured the relative signal intensity (SI) and relative contrast because all images were obtained with a parallel imaging technique[22]. The signal intensities were determined for the cartilage, joint fluid in the medial femoral neck pouch, acetabular bone, and labrum of the right hip of the control group(Fig.2). The signal intensities were measured in the sagittal plane through the femoral head in the original image of 3D FSE-Cube (3D FSE-Cube org), in the oblique coronal plane of the 3D FSE-Cube image equivalently reformatted to 2D FSE-radial sequence(3D FSE-Cube mpr), and in the plane of 0 degrees on the 2D FSE-radial image, using software(Osirix; http://www.osirix.com/). The relative SI of each structure was calculated by dividing the SI by the standard deviation(SD). The relative contrast of structure A(a) to structure B(b) was calculated as (SIa-SIb) /(SDa2+SDb2)1/2. We measured the joint fluid to cartilage, joint fluid to labrum and bone to labrum relative contrast. Measurements were performed by a single orthopedic surgeon(S.H.) with 9 years of experience in image analysis.
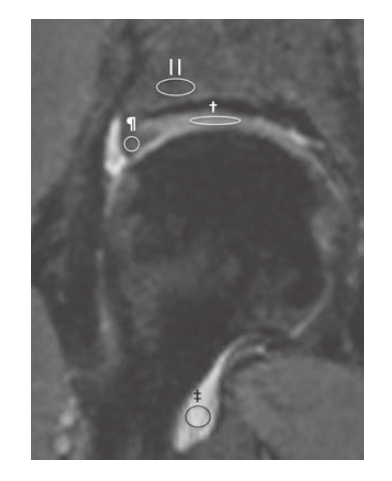
Fig. 2
The 3D-FSE Cube image demonstrating the example of ROIs on the cartilage(†), joint fluid (‡), acetablar bone(||), and labrum(¶) in the hip joint for the measurement of signal intensities.
For the qualitative analysis, we evaluated artifacts, image blur, and overall quality as previously reported [22]. Analysis was performed by a musculoskeletal radiologist and an orthopedic surgeon(S.T. with 16 years of experience in image analysis and S.H.) blinded to the subject and sequence information. Artifacts were assessed using a 5-point scoring system; 5: no artifacts, 4: mild artifacts, 3: moderate artifacts, 2: severe artifacts, and 1: unreadable study. Image blur was assessed using the following scale; 5: sharp, 4: mild-blur, 3: moderateblur, 2: severe-blur, and 1: unreadable. Overall quality was assessed using the following scale; 5: excellent, 4: good, 3: satisfactory, 2: poor, and 1: non-identified. The mean values of the two readers were calculated and compared between the 3D FSE-Cube and 2D FSE-radial sequences.
For inter- and intra-observer reliability, we followed the methodology of Takazawa et al[23]. Before the trials, three orthopedic hip surgeons(S.H., J.N., and S.K; with 9, 14, 17 years of experience in image analysis) were provided with detailed instructions regarding Abe’s classification systeml[10]and were asked to classify the shape and grade of the labral lesion group independently without any clinical information. The shape of the labrum was classified into four types(for a triangular shape, the point was well defined; for a round shape the edge was well-rounded; for absent there was almost no evidence of shape; all other shapes fell into the irregular group). The signal intensity change of the labrum was classified into five grades(homogeneous, low signal intensity images were classified as Grade 1; moderate signal intensity in the intralabral area was classified as Grade 2A; high signal intensity in the intralabral area as Grade 2B; high signal intensity that communicated with the free surface as Grade 3A; and diffuse high signal intensity in the whole area as Grade 3B). We reformatted the 3D FSE-Cube images to the equivalent plane as 2D FSE-radial images and evaluated the shape of the labrum. Reformatting was performed by a single reader(S.H.), so that each reader could classify in the same plane. To evaluate the intra-observer reliability, a second trial was performed in a similar fashion 4-5 weeks later, with the MR images in a different order.
Statistical analysis was performed using commercial software(SPSS 16.0, IBM, Chicago, IL). The 3D FSE-Cube org, 3D-FSE Cube mpr, and the 2D FSEradial image were compared with respect to cartilage, joint fluid, and labrum relative SI and the joint fluid to cartilage, joint fluid to labrum and bone to labrum relative contrast in the control group by one way repeated measures analysis of variance (ANOVA) followed by Bonferroni correction for multiple comparisons. Artifacts, image blur, and overall quality were analyzed using a Wilcoxon signed-rank test. A P-value of less than 0.05 was considered significant. Cohen’s quadratic weighted kappa was used to assess the inter- and intra-observer reliability. A kappa of 0.21- 0.40 was considered to be fair; 0.41-0.60, moderate; 0.61-0.80, substantial; and 0.81-1.0, excellent.
The results of the quantitative assessment are shown in Figures 3 and 4. The mean values of the relative SIs of the cartilage were 8.1, 9.1 and 9.5 in the 3D FSECube org, 3D-FSE Cube mpr, and 2D FSE-radial, respectively. The mean relative SIs of the joint fluid were 12.5, 13.4 and 11.4 and those of the labrum were 3.3, 2.9 and 4.1 respectively. There were no significant differences between the relative SIs of the evaluated sequences. The mean values of the relative contrast are shown in Figure 4. The mean relative contrasts of the joint fluid to cartilage were 5.6, 5.9 and 1.2 in the 3D FSE-Cube org, 3D-FSE Cube mpr, and 2D FSE-radial, respectively. The joint fluid to labrum mean relative contrasts were 9.3, 9.2 and 5.1 and those of the bone to labrum were 0.2, 0.3 and 1.1 respectively. The 3D FSECube org and mpr were significantly higher than that of the 2D FSE-radial in the joint fluid to cartilage relative contrast and the joint fluid to labrum(p=0.002, p= 0.000002, respectively)(Fig. 4, 5). There were no significant differences in the relative contrast of the bone to labrum on the evaluated sequences.
The results of the qualitative analysis are shown in Table 1. The 2D FSE-radial sequence produced significantly higher scores than the 3D FSE-Cube sequence in image blur and overall quality(P=0.003 and 0.0002, respectively). There was no significant difference in artifacts between each sequence.
The frequency of Shape and Grade classifications in all labral segments of the labral lesion group is shown in Table 2. The frequency of appearance was almost same in each sequence. For inter- and intra-observer reliability, the weighted kappa of each classification is shown in Table 3. Both the 3D FSE-Cube and 2D FSE-radial sequences showed excellent inter- and intra-observer reliabilities in the Shape and Grade classifications(Fig. 6).
Fig. 3
Bar graph shows comparison of relative Signal Intensity(SI) in cartilage, joint fluid and labrum between 3D-FSE Cube org, mpr and 2D-FSE radial imaging. There were no significant differences between each imaging in all structures.
Fig. 4
Bar graph shows comparison of relative contrast in joint fluid to cartilage, joint fluid to labrum and bone to labrum between 3D-FSE Cube org, mpr and 2D-FSE radial imaging. Relative contrast was significantly higher in 3D-FSE Cube org and mpr than 2D-FSE radial in joint fluid to cartilage and joint fluid to labrum(p=0.002, p=0.000002, respectively).
Fig. 5
A 34-year-old woman in the control group with increased joint fluid to labrum contrast in 3D-FSE Cube.
(a) 3D-FSE Cube original image.
(b) 3D FSE-Cube image reformatted accordant with 2D-FSE radial.
(c) 2D-FSE radial image of 30 degrees anteriorly sectioned.
Fig. 6
A 25-year-old woman in labral lesion group with every readers agreement. Shape was round and grade was 3A.
(a) 3D FSE-Cube image reformatted accordant with 2D-FSE radial.
(b) 2D-FSE radial image of 30 degrees anteriorly sectioned.
Table. 1
Mean subjective scores of artifacts, image blur, and overall quality on the 2D FSE-radial and 3D FSECube sequences
Table. 2
The frequency of Shape and Grade classifications
Table. 3
Inter- and intra-observer reliability of shape and grade classifications
The labrum has a triangular shape when viewed in cross-section, and is approximately 2 to 3 mm thick [24]. In DDH, a labral lesion is thought to originate in the antero-superior portion of the acetabulum[4]. In FAI, a labral lesion of a cam-type impingement is likely to occur at the transition-zone, and a lesion of a pincertype is likely to occur intra-substance before a chondral injury[25]. The location of a labral lesion differs from the pathology three-dimensionally, so Ziegert et al claimed that the detection of labral tears was optimal with a combination of three sequences(coronal T2- weighted with fat saturation, axial oblique T1-weighted with fat saturation, and sagittal T1-weighted with fat saturation)[12]. A radial sequence obtained through the center of the acetabulum is the established method to evaluate an anatomic abnormality of the labrum[10]. In an additional study, Takazawa reported that the radial sequence had high intra- and inter- reliability[23]. In our study, a similar performance for the evaluation of the labrum was shown for each sequence. However, in the 2D-FSE radial sequence, the interval of each angle was impossible to evaluate. So, the ability to reformat images to arbitrary planes is an advantage of the 3D-FSE Cube sequence.
The availability of a multi-plane, post-processing, and reformatted image is an advantage of a 3D isotropic voxel sequence[16]. In our study, the original and reformatted images from the 3D-FSE Cube sequence had the same signal intensity and contrast. Studies comparing conventional 2D and isotropic 3D image quality are controversial. Stevens et al reported an equivalent quality of the 3D FSE-Cube and conventional 2D FSE sequences for the ankle[26]. For the knee, Kijowski and Ai reported that the 3D FSECube sequence has a similar or superior image quality as that of the 2D FSE sequence in comparison with arthroscopic results [27,28], and Chen et al reported that the 3D FSE-Cube sequence produced high image quality in a signal-to-noise/contrast-to-noise comparison of six new 3D MR methods for evaluating knee cartilage[16]. The 3D FSE-Cube sequence demonstrated an inferior score in the qualitative evaluation in our study, which is likely due to the acquisition of high spatial frequencies late in the echo train[27]. However, this decrease did not affect the morphological evaluation of the labrum. A thin slice thickness is an advantage of the 3D-FSE Cube sequence for the evaluation of such a small structure. In the present study, the slice thickness of the 3D-FSE Cube image is 0.9mm, which can avoid partial volume effects. The imaging time with the 3D FSE-Cube sequence is slightly longer than that of the conventional 2D FSE sequence. However, complex registration is not needed because images can be subsequently reformatted in multiple planes.
MR arthrography versus non-contrast MRI of the labrum is still controversial. Czerny et al reported accurate detection of labrum tears in comparison with surgical findings[14]. Recent research has supported the superior accuracy of MR arthrography. Byrd and Toomayan reported a higher sensitivity and specificity of MR arthrography compared to non-contrast MRI using arthroscopy as the definitive diagnosis[29,30]. This superiority is thought to be due to an increased signal intensity of the joint fluid against the low signal intensity of the normal labrum[30]. On the other hand, in the similar study, Mintz et al reported a high reliability of non -contrast MRI for labral tears [31]. In a meta-analysis study, Smith et al concluded that both MRI and MRA may be useful adjuncts in the diagnosis of acetabular labral tears in adults[32]. In our study, increased relative contrast in the joint fluid to labrum due to fat suppression may improve the diagnostic accuracy for labrum tears.
Our study has several limitations. We did not compare the MR results with the arthroscopy as a reference standard. So we could not calculate the sensitivity and specificity of the radiographic findings. However, our study demonstrated a similar image quality for the 3D-FSE Cube and the 2D-radial FSE sequences. Another limitation was the small patient population. However, the Cohen’s quadratic weighted kappa was almost identical, and a larger number will not change the statistical evidence.
In conclusion, the present study has demonstrated that a 3D-FSE Cube sequence at 3T has a similar image quality compared to conventional 2D-FSE imaging. Considering the enhanced ability to reformat images, the addition of a 3D-FSE Cube acquisition to the routine imaging protocol may improve the diagnosis of hip labral tears. Further prospective studies with MR arthroscopy are needed to verify the accuracy of this sequence.
The co-author, Junichi Nakamura, received JSPS KAKENHI Grant Number 25870125 for this work. The other authors do not receive any financial support or other benefits from commercial sources for the work.
Address correspondence to Dr. Shigeo Hagiwara.
Department of Orthopaedic Surgery, Graduate School of Medicine, Chiba University, 1-8-1, Inohana, Chuou-ku, Chiba 260-8670, Japan.
Phone: +81-43-226-2117. Fax: +81-43-226-2116.
E-mail:karakaze2000jp@yahoo.co.jp
