




Chiba Medical J. 94E:51-54,2018
doi:10.20776/S03035476-94E-5-P51
[ Case Report ]
Naoki Shimizu1), Shinjiro Horikawa1),
Osamu Saito1)and Yukihiro Hasegawa2)
1 ) Department of Pediatric Emergency & Critical Care Medicine, Tokyo Metropolitan Children’s Medical Center, Tokyo 183-8561 .
2 ) Department of Endocrinology, Tokyo Metropolitan Children’s Medical Center, Tokyo 183-8561 .
(Received May 7, 2018, Accepted August 1, 2018)
Increased intracranial pressure with cerebral herniation is a devastating but preventable complication of diabetic ketoacidosis encountered in pediatric critical care. Children with severe diabetic ketoacidosis(DKA) always present an extremely low partial pressure of arterial carbon dioxide(PaCO2) value at presentation; however, the cerebral blood volume increases rather than decreases, leading to brain edema. The cerebrovascular pathophysiology of children with DKA is still unclear. We report here the use of near infrared spectroscopy in our critical care unit to measure regional oxygen saturation(rSO2) and investigate cerebrovascular reactivity against PACO2 in children with DKA. The data presented here demonstrate a favorable relationship between the treatment course of DKA and the normalization of rSO2 and PACO2. This case showed high rSO2 although the PACO2 was abnormally low, despite the fact that a low PACO2 usually indicates low rSO2 due to cerebral vasoconstriction. This phenomenon illustrates an abnormal condition in cerebral vessel physiology which resolves within 24-48 hours of initial treatment for DKA.
Pediatric, Brain edema, Mortality, Neuro-monitoring, Ultrasound
Increased intracranial pressure(IICP) with cerebral herniation is a devastating but preventable complication of diabetic ketoacidosis still encountered in pediatric critical care[1,2]. Partial pressure of arterial carbon dioxide(PACO2) is one of the determinants of cerebral blood flow and usually lowers the ICP when decreased[3]. However, children with severe DKA always have extremely low PACO2 at presentation yet are at increased risk of cerebral edema. The cerebrovascular pathophysiology of children with DKA is still unclear.
Near infrared spectroscopy(NIRS) is widely used for non-invasive and continuous brain oxygenation monitoring in neurological critical care[4-6]. NIRS was originally described as a novel monitoring device for relative changes in the intracranial chromopher levels of oxyhemoglobin(O2Hb) and deoxygenated hemoglobin(HHb). Excellent correlation between NIRS data and cerebrovascular phenomena has been reported, such as intracranial hemorrhage, vasospasms, increased intracranial pressure, etc.
We report here the use of NIRS in our ICU to investigate cerebrovascular reactivity against PACO2 in children with DKA.
A 1-year-old boy was transferred to our institution from a local hospital with the tentative diagnosis of DKA. His data showed severe metabolic acidosis(pH 6.9, PACO2 22 mmHg, HCO3 -5 mmol/L, BE -28 mmol/L) and a high blood glucose level(over 1,000 mg/dL). She was lethargic(GCS 7, E2V1M4) and showed significant tachypnea(RR 45/minute Kussmaul breathing pattern) and compensated shock(HR 186/ min, capillary refilling time 3 seconds). DKA was diagnosed, and she was admitted to our pediatric ICU.
We started NIRS assessment soon after the patients’ ICU admission. INVOSTM(Medtronic) was used in our institution. The optodes were placed on the forehead of the patient’s frontal scalp. The distance of optodes, signal strength and the differential pathlength factor(DPF) etc. were adjusted automatically in INVOSTM, and we just need to place the ready-made sensor on patient’s forehead. The regional SO2 (rSO2) were measured continuously by INVOSTM. An arterial line was inserted and frequent measurements of blood gas were taken by bed-side pediatric intensivists. The rSO2 and arterial blood gas values were measured and recorded simultaneously.
The rSO2 values measured by INVOSTM and PACO2 values measured by arterial blood gas analysis are shown in Figure 1. At admission to the ICU, arterial blood gas analysis showed a very low PACO2 compensating for the deep metabolic acidosis caused by DKA onset. Normally, a low PACO2 induces brain vasoconstriction and usually indicates a low rSO2. However, despite his low PACO2 value, INVOSTM showed a very high rSO2 suggesting brain vasodilation and high cerebral blood flow.
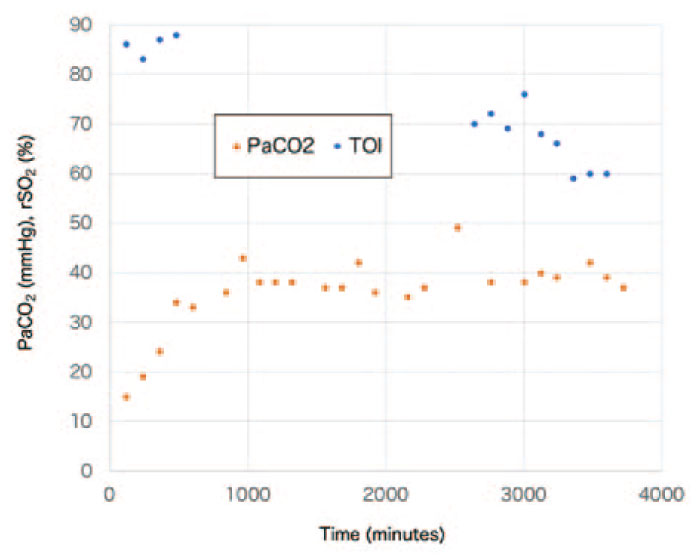
Fig. 1
rSO2 values detected by INVOSTM and PACO2 values measured by arterial blood gas analysis
In addition, CAT scan was performed in this patient before the ICU admission and cerebral blood flow was measured by transcranial Doppler(TCD) soon after the ICU admission(Figure 2; CAT scan, Figure 3; TCD). CAT scan indicated mild brain edema, and TCD illustrated the abnormal blood flow pattern(high systolic and low diastolic pattern meaning high pulsatility/ resistive index) both were suggesting increased ICP. These facts explained clinical backgrounds of high rSO2 value initially indicated in this case soon after the ICU admission.
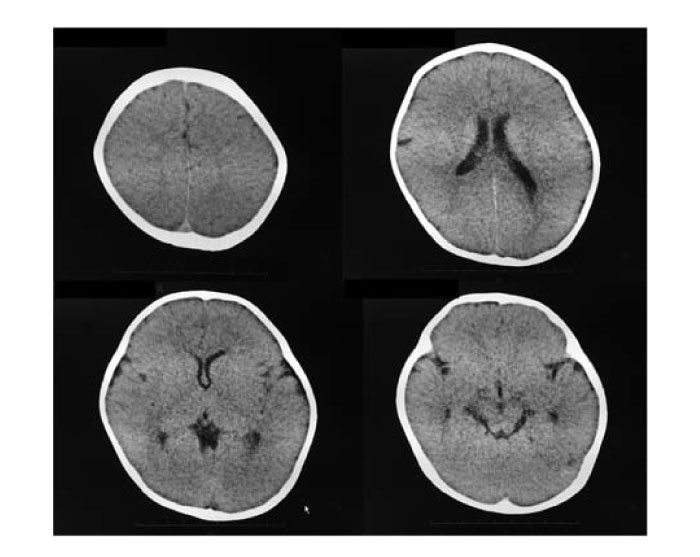
Fig. 2
CAT scan before the ICU admission
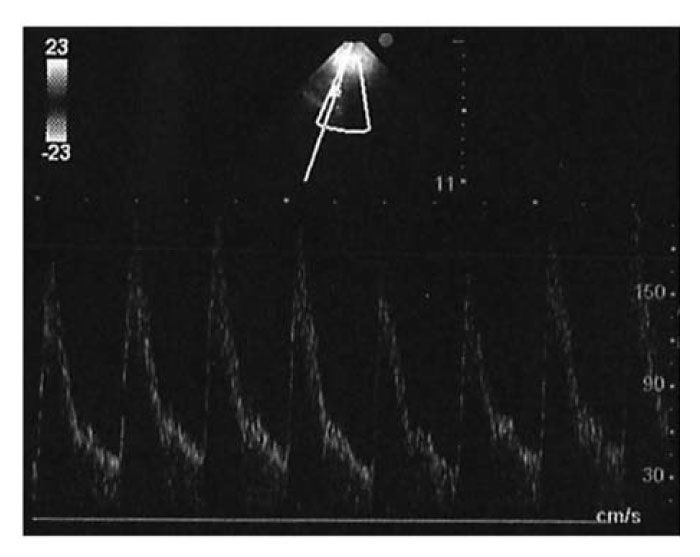
Fig. 3
TCD after the ICU admission
Although diabetic ketoacidosis(DKA) is a common pediatric emergency for which effective treatment is available, we still see neurological complications associated with the initial treatment of this disease. Cerebral edema is an uncommon but devastating complication of DKA in children. However, the pathophysiology of acute neurological complications of DKA are not completely understood.
Glaser et al. conducted a multicenter study investigating the risk factors for cerebral edema in DKA and concluded that children with DKA who have low PACO2 and high serum urea nitrogen concentrations at presentation and are treated with bicarbonate are at increased risk of cerebral edema[1]. Abnormal PACO2 is one of the major factors of neurological complications of DKA. According to Glaser et al., neurological deterioration commonly occurs within 0-24 hours after the initiation of treatment.
Based on TCD data, Hoffman et al. reported that the cerebral vasculature reacts differently in the early phase of DKA treatment[7,8]. Within 0-12 hours after initiating treatment, the cerebral vascular tone becomes blunted in response to the low PACO2. The time frame in which this occurs coincides with the most common period of neurological deterioration in DKA. During the treatment for DKA, PACO2 recovers and cerebrovascular CO2 reactivity normalizes within 24 hours; then the cerebral vasoparalysis resolves completely within 48 hours.
Normally, PACO2 is one of the determinants of cerebral blood flow(CBF) and cerebral blood volume(CBV), both of which control intracranial pressure(ICP). However, the transient phenomenon of the type reported here can cause the CBF to increase during the initial DKA treatment and thereby augment the risk of increased ICP particularly in the first 24 hours after the start of DKA treatment.
CBF can be measured or estimated in several ways. Although the Xenon-CT is the gold standard, it is not feasible in an acute care setting such as the emergency department and/or critical care unit where DKA patients are usually treated. Jugular venous oxygen saturation(SjvO2) has been used clinically to estimate changes in the CBF[9]. The SjvO2 catheter is useful in some clinical settings, but its use with DKA patients is still considered to be“ invasive”. Given these considerations, NIRS has come to be widely used as a“ non-invasive” method of continuous neuro-monitoring in the critical care setting.
Our data demonstrated a good relationship between the treatment course of DKA and normalization of rSO2 and PACO2. All the patients showed high rSO2 although their PACO2 was abnormally low, despite the fact that low PACO2 usually indicates low rSO2 due to cerebral vasoconstriction. This abnormality of cerebral vessel physiology normalizes within 24-48 hours of initial treatment of DKA.
The present study is the first report of abnormal cerebrovascular reactivity studied with NIRS. More data are needed to investigate the correlation between the findings of NIRS and other methods designed to measure CBF/CBV. Our knowledge of the cerebrovascular pathophysiology of children with DKA is still uncertain, and further research is needed to improve the outcomes of acute phase DKA.
NS, SH, and OS managed the case. SH measured TCD. YH provided endocrinology input to the patient’s care. NS, SH, OS, and YH contributed to writing of the report. Consent to publication was obtained from the family. Publication was approved by the Institutional Review Board of Tokyo Metropolitan Children’s Medical Center. Authors thank Mr. James Robert Valera for his assistance with editing the manuscript.
Address correspondence to Dr. Naoki Shimizu.
Department of Pediatric Emergency & Critical Care Medicine, Tokyo Metropolitan Children’s Medical Center, 2-8-29, Musashidai, Fuchu, Tokyo 183-8561, Japan.
Phone: +81-42-300-5111. Fax: +81-42-312-8160.
E-mail:naoki_shimizu@mac.com
