




Chiba Medical J. 95E:1-5,2019
doi:10.20776/S03035476-95E-1-P1
[ Original Article ]
Naoki Shimizu1), Louis Akiyama1), Kazunori Imai1,2),
Norihisa Miyashita1,3), Naoto Mizushiro1,4), Takanari Ikeyama1,2),
Hiroshi Kurosawa1,3), Osamu Saito1), and Ichiro Watanabe1,5)
1 ) Department of Pediatric Emergency & Critical Care Medicine, Tokyo Metropolitan Children’s Medical Center, Tokyo 183-8561 .
2 ) Department of Critical Care Medicine, Aichi Children’s Health and Medical Center, Aichi 474-8710 .
3 ) Department of Pediatric Critical Care Medicine, Hyogo Prefectural Kobe Children’s Hospital, Hyogo 650-0047 .
4 ) Department of Pediatrics, Aizawa Hospital, Nagano 390-8510 .
5 ) Children’s Hospital of Philadelphia, USA.
(Received July 31, 2018, Accepted August 2, 2018, Published February 10, 2019.)
Background: Propofol infusion syndrome(PRIS) is characterized by lactic acidosis, rhabdomyolysis, and circulatory collapse after several days of high-dose propofol infusion. PRIS typically affects young and critically ill patients and is a potentially fatal cardiovascular and metabolic condition. On the contrary, short period intravenous drip and intermittent intravenous administration of propofol are commonplace in the operating theatre, however, there are no biochemical data indicating the safety of these settings in Japanese children.
Methods: Thirty consecutive children who were admitted to the pediatric intensive care unit(PICU) after elective neurosurgical surgery and anesthetized by propofol infusion were enrolled. The total dosage and average speed of propofol infusion during the operation was calculated. The serum lactate level, blood gas analysis including the pH, bicarbonate, base excess, and electrolytes were assessed postoperatively.
Results: The total dosage of propofol administered during surgery was 53.8(37.4-71.1) mg/kg. The average speed of Propofol infusion administered during surgery was 9.9(8.6-11.9) mg/kg/hr. No case of PRIS or mortality occurred among these patients. All the patients had normal serum lactate and potassium levels. The blood gas pH was normal in most samples, but the bicarbonate and base excess were slightly low. However, there was no statistically significant difference in the total dose or average speed of propofol administration except for the lower bicarbonate level related to the higher average infusion speed of propofol.
Conclusion: Our observational study revealed that the maximum mean rate of 9.9 mg/kg/hr and a total dosage of 53.8 mg/kg did not induce PRIS or death, did not elevate the serum lactate or potassium level, and slightly decreased the blood gas pH. The base excess was unaffected by the propofol dosage/ speed of infusion. More data are required to establish the safety parameters for propofol administration and guidelines for propofol use in Japanese children.
Propofol infusion syndrome, Metabolic acidosis, Sudden death, Pediatric intensive care unit, Anesthesia
The propofol infusion syndrome (PRIS) is a potentially fatal cardiovascular and metabolic condition that has been described in both pediatric and adult patients sedated with propofol. Although many reports on PRIS have been published since 1992[1], the clinical features and pathophysiology of this condition remain uncertain[2-5]. Recently, PRIS attracted serious concern in Japan and gave impetus to changes in pediatric critical care.
PRIS is characterized by lactic acidosis, rhabdomyolysis, and circulatory collapse after several days of high-dose propofol infusion. The patients are typically young and critically ill, and the mortality rate is high[6-13]. However, several studies have also shown cases with no change in the lactate level, suggesting that shortterm use/low-dosages of propofol may be safe[14-16]
Due to a recent PRIS-related incident in Japan, the intermittent or short-term use of propofol in the pediatric critical care setting tends to be discouraged. However, the avoidance of propofol may deprive sick children of the benefits of this useful anesthetic agent.
This study examined the effect of propofol on serum lactate, blood gas, and electrolytes in patients admitted to the pediatric intensive care unit(PICU) after a long surgical procedure during which propofol was used as an anesthetic agent.
Thirty consecutive pediatric patients(2 to 10 years old) admitted to the PICU at the Tokyo Metropolitan Children’s Medical Center(TMCMC) between April 2013 and March 2014 for elective neurosurgery using a propofol infusion as an anesthetic and those with an arterial line in place were enrolled. Congenital metabolic diseases and hemodynamic instability during surgery were the exclusion criteria but applied to none of the patients.
After admission to the PICU, the arterial lines were kept in place, and arterial blood gas samples were drawn from the lines in accordance with the usual clinical practice including the time of admission in all the children. The blood gas analysis including lactate and electrolytes was done using ABL 800 Flex (Radiometer).
The serum lactate level, blood gas analysis including the pH, base excess, bicarbonate, and electrolytes were assessed. The total dosage and average speed of infusion of propofol during surgery were calculated and compared between the normal biochemical group (lactate=<2, potassium=<4.5, pH>=7.36, base excess>=-2, bicarbonate>=22) and abnormal biochemical group(lactate>2, potassium>4.5, pH< 7.36, base excess<-2, bicarbonate<22). Student’s T-test was done, and p<0.05 was defined as statistically significant.
This study was approved by the ethics board of the Medical Research Committee of Tokyo Metropolitan Children’s Medical Center(TMCMC). Publication was approved by the Institutional Review Board of TMCMC.
Thirty cases were enrolled, and 94 blood samples were drawn from the arterial lines. The case characteristics are shown in Table 1. The total dosage of propofol administered during surgery was 53.8(37.4- 71.1) mg/kg. The average speed of propofol infusion during surgery was 9.9(8.6-11.9) mg/kg/hr. No case of PRIS or mortality occurred.
The serum lactate and potassium levels were normal in all the patients(median serum lactate level: 0.7(0.6- 1.1) mmol/L, potassium: 3.6(3.4-3.9)). The blood gas pH remained normal in most samples(93%)(Table 2). The base excess and bicarbonate were in the low range(<-2, <22 mmol/L, respectively) in 41% of the samples, but there was no statistically significant difference in the total dose or average speed of propofol infusion. However, the bicarbonate level related to the higher average infusion speed of propofol was significantly low(Table 3,Table 4).
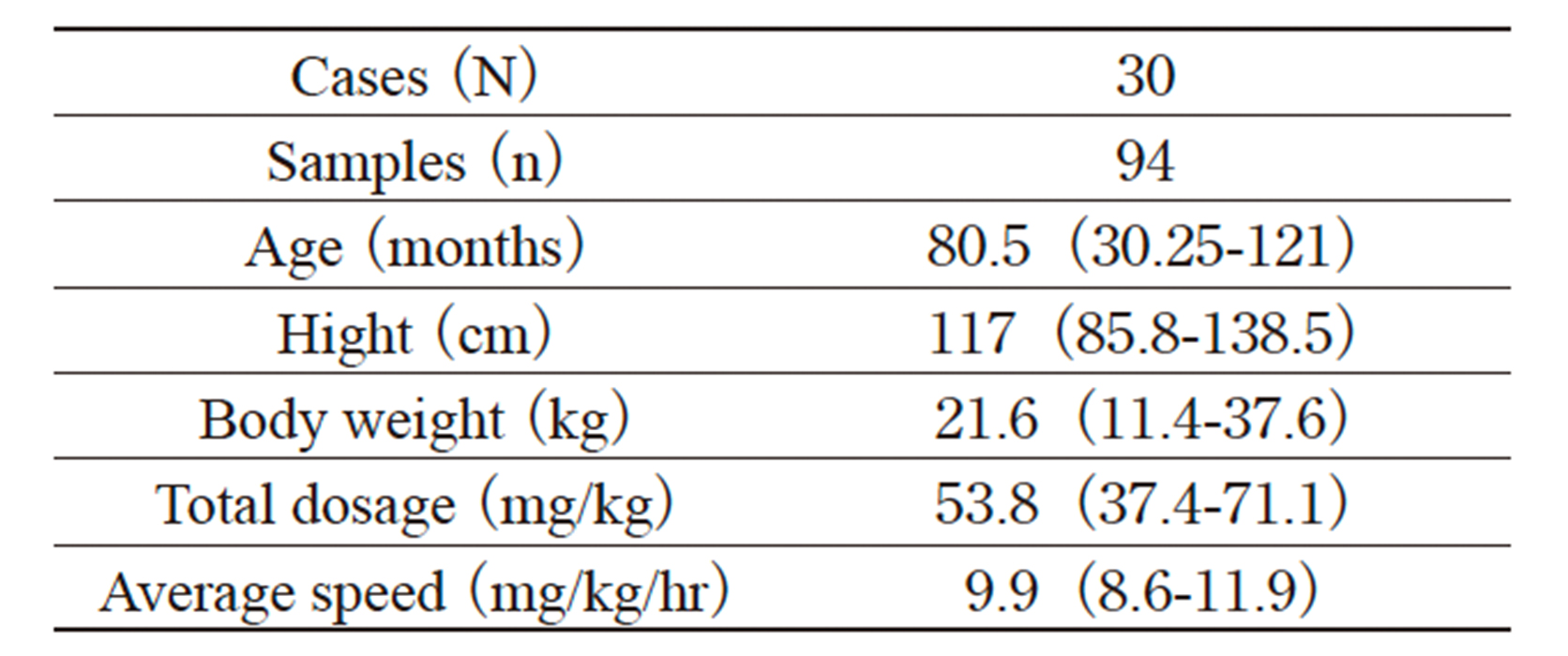
Table. 1 Characteristics of the cases
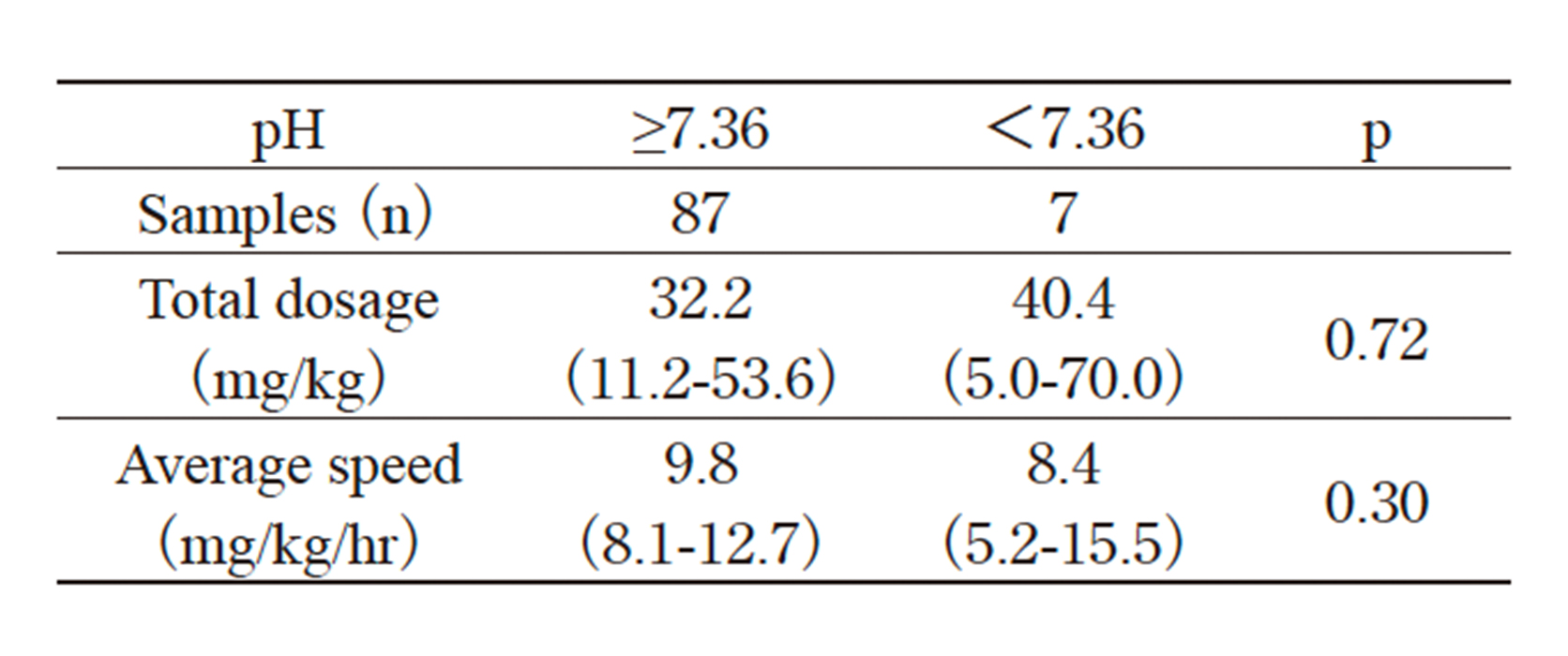
Table. 2 Change in pH after propofol administration during surgery
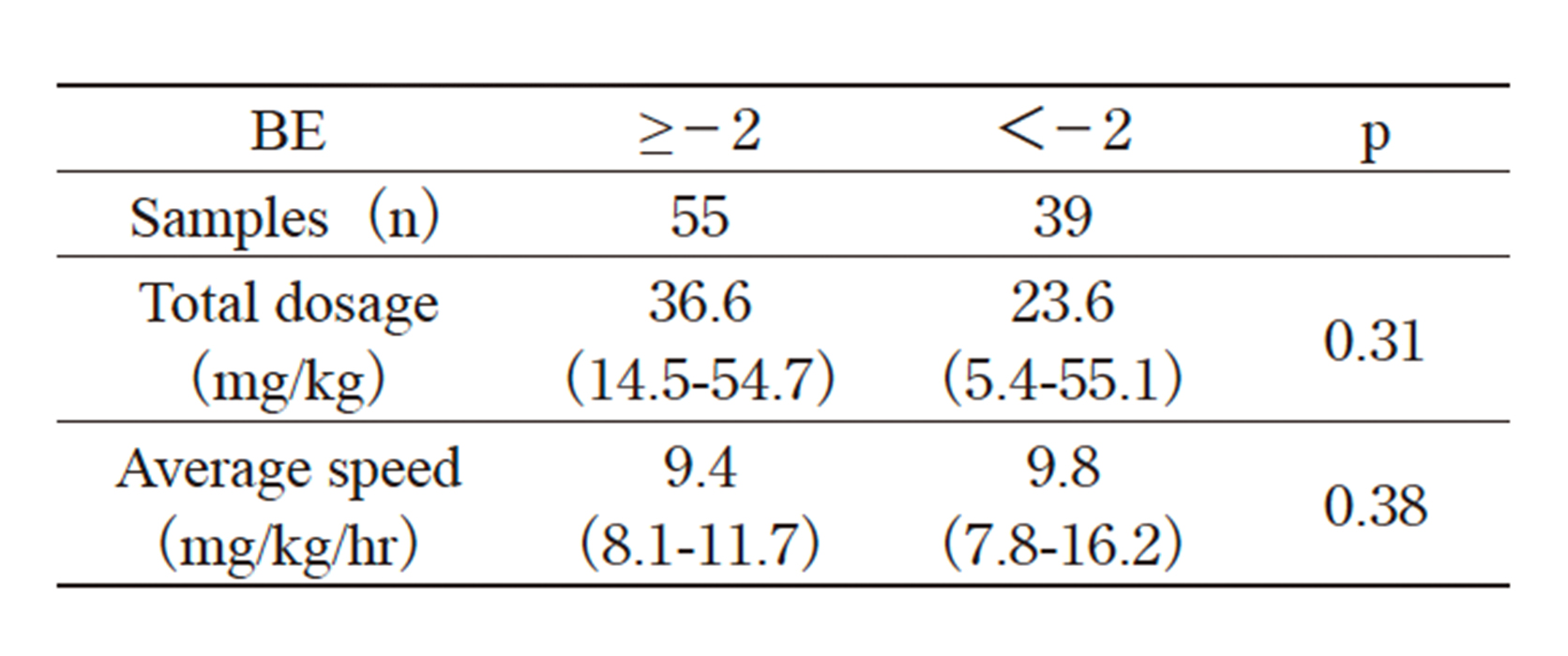
Table. 3 Change in bicarbonate after propofol administration during surgery
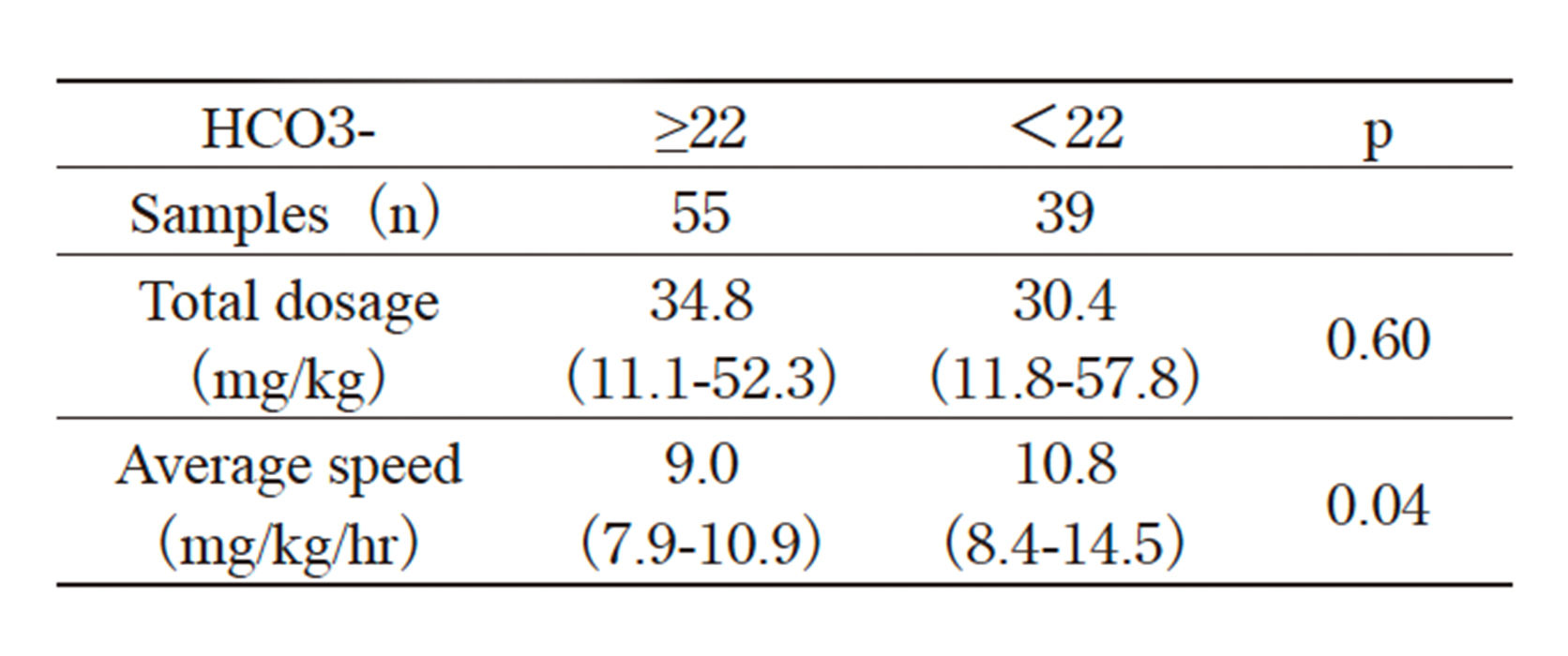
Table. 4 Change in base excess after propofol administration during surgery
The use of propofol as a sedative for artificial ventilation for children in the intensive care unit(ICU) was prohibited in Japan when it was determined that indications for the use of the agent were not backed by sufficiently robust scientific evidence(despite intraoperative use in children being allowed). There are several standards and / or clinical guidelines of propofol use for children in PICUs outside Japan[17-19].
A maximum mean rate of 4 mg/kg/hr and maximum duration of 24 hours(total dosage around 100 mg/ kg) are the standard limitations on propofol infusions for children in the PICU[15,16]. A recent report by the Ministry of Health, Labour and Welfare of Japan recommended a maximum rate of 4 mg/kg/hr and maximum duration of 48 hours with close blood examination and monitoring[20].
In the medical treatment of children, drugs are used outside the boundaries of approved licensing, for example under the terms of off-label use. However, this requires critical reasoning and experience with the drug involved. Our observational study revealed that a maximum mean rate of 9.9 mg/kg/hr and total dosage of 53.8 mg/kg did not induce PRIS or death, did not elevate the serum lactate nor potassium levels, and slightly decreased blood gas pH, while the base excess was unaffected by propofol dosage/speed of infusion.
This study has several limitations including the small number of cases and samples(30 cases, 94 samples), the fact that it was a single-center study, homogeneity of the subjects (those with only postneurosurgical procedures), retrospective model, etc. However, this is the only study to reveal the biochemical characteristics of children after a propofol infusion.
Propofol is used worldwide intravenously to induce and maintain anesthesia in procedural and critical care sedation for children[21-24]. Continuous infusion for sedation in the PICU is controversial due to the risk of PRIS; however, complete prohibition of its use is uncommon. With strict monitoring of, and limits on, its use, continuous infusion is allowed in several countries. Intermittent use of propofol is usual practice and not a cause of concern.
Due to the public outcry caused by the PRIS-related incident in Japan, many physicians and institutions have become reluctant to use propofol even intermittently or for procedural sedation in the critical care and emergency department settings. However, such a practice may deprive sick children of the benefits of this anesthetic agent. More data are needed to establish the safety range for propofol administration and guidelines for propofol use in Japanese children.
NS and IW conceived and designed the study. KI and NM are involved in data collection. NS, KI, NM, and IW analyzed and interpreted the data. NS, NM, TI, HK, OS, and IW were involved in development, review, and approval of the manuscript.
We thank Mr. James Robert Valera for his assistance with editing the manuscript.
The authors declare that they have no conflicts of interest with regard to the content of this article.
Address correspondence to Dr. Naoki Shimizu.
Department of Pediatric Emergency & Critical Care Medicine,
Tokyo Metropolitan Children’s Medical Center, 2-8-29,
Musashidai, Fuchu, Tokyo 183-8561, Japan.
Phone: +81-42-300-5111. Fax: +81-42-312-8160.
E-mail: naoki_shimizu@mac.com
