




Chiba Medical J. 95E:7-9,2019
doi:10.20776/S03035476-95E-1-P7
[ Case Report ]
Naoki Shimizu, Shigetoshi Ogiwara, and Osamu Saito
Department of Pediatric Emergency & Critical Care Medicine, Tokyo Metropolitan Children’s Medical Center, Tokyo 183-8561 .
(Received May 11, 2018, Accepted August 1, 2018, Published February 10, 2019.)
Advanced warning of desaturation based on child-specific physiology is needed. Pulse oximetry does not indicate downward trends in arterial partial pressure(PaO2) until the percutaneous arterial oxygen saturation(SpO2) begins to fall. Therefore, SpO2 cannot provide advanced warning of desaturation events. The oxygen reserve index(ORI) is a new, noninvasive method of monitoring oxygen reserves. The clinical usefulness of the ORI has been reported in anesthesiology but reports from pediatric critical care are still few in number. The current study is the first to demonstrate the usefulness of the ORI for the management of sick children in a pediatric intensive care unit. To improve outcomes for sick children, using the ORI for advanced warning of desaturation is recommended.
oxygen reserve index, children, anesthesia, sedation, functional residual capacity, risk management
Over 40 years have passed since the introduction of pulse oximetry by Aoyagi et al.[1-3]. Despite its significance, pulse oximetry does not indicate downward trends in arterial partial pressure (PaO2) until the percutaneous arterial oxygen saturation(SpO2) begins to fall. Thus, this technology is limited by the fact that SpO2 cannot provide advanced warning of desaturation events.
The oxygen reserve index (ORI) is a new, noninvasive method of monitoring the oxygen reserve, such as the PaO2 level above an SpO2 of 100%. The ORI is a pulse oximeter-based nondimensional index that ranges from 1 to 0 as arterial partial pressure(PaO2) decreases from around 200 to about 80 mmHg and is measured by optically detecting changes in venous saturation(SvO2) after arterial saturation(SaO2) has reached the maximal level.
The clinical usefulness of the ORI has been reported in anesthesiology[4-7], but reports from pediatric critical care field are few in number. The current study is the first to demonstrate the usefulness of the ORI for sick children in a pediatric intensive care unit(PICU).
Case 1: A 1-year-old boy was intubated and ventilated due to retropharyngeal abscess. He was admitted to our PICU. After the stabilization, we performed naso-tracheal intubation on the assumption that artificial ventilation would be required for several days. We used the ORiTM (MASIMO, Japan) in conjunction with SpO2 monitoring(Fig. 1). During the procedure, before the drop in the SpO2,(③) we noticed a drop in the ORI reading(①). We stopped the procedure and re-oxygenated him(②) and later re-attempted intubation. The desaturation event was minimized, and the procedure was completed safely.
Case 2: A 1-year-old boy was admitted to our PICU with pulmonary hypertension(PH). We used the ORiTM with SpO2 monitoring(Fig. 2). Before desaturation caused by a PH attack(③), we observed a drop in the ORI(①), based on which we were able to oxygenate this patient slightly earlier than is normally possible (②). The desaturation event was relatively mild and was prevented from becoming more serious.
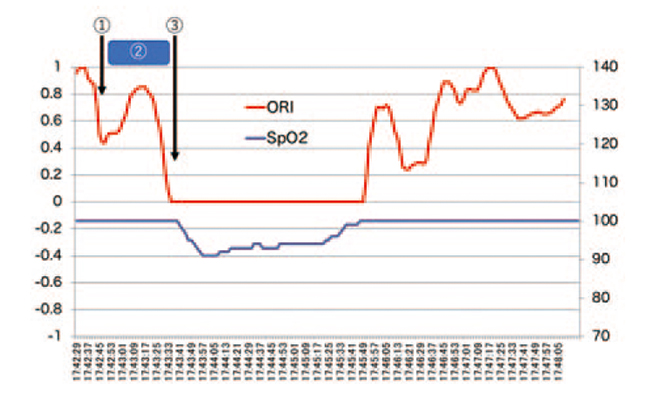
Fig. 1
Trend in the ORI and SpO2 during nasopharyngeal end-tracheal intubation
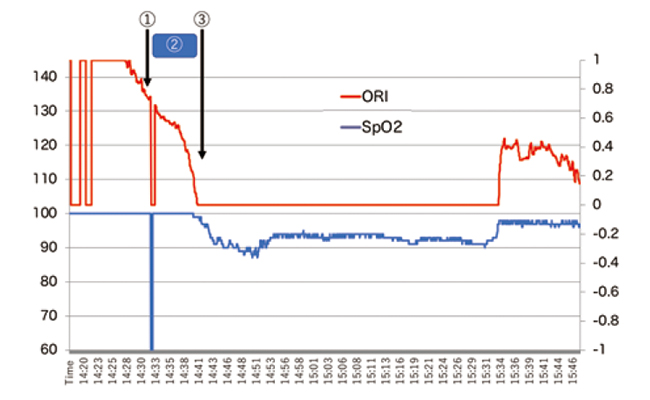
Fig. 2
Trend in the ORI and SpO2 during the management of a case with pulmonary hypertension
Cardiac arrest or bradycardia are serious complications of hypoxia during patient management in the PICU. To prevent these potentially fatal outcomes, monitoring devices are always useful; however, we need to realize the limitations of these devices.
Pulse oximetry based on SpO2 measurements is one of the most useful monitoring tools in the PICU; however, venous pulsation may become more prominent in situations with lower perfusion or massive body movement. The very limited performance of pulse oximetry under these conditions has presented a major clinical problem[8]. Furthermore, pulse oximetry is unable to indicate downward trends in the PaO2 until the SpO2 begins to fall. Thus the SpO2 cannot provide advanced warning of desaturation events [6].
Functional residual capacity(FRC) is one of the determinants of oxygenation[9]. For reasons having to do with child physiology, FRC in children is smaller than in adults and prone to faster desaturation[10,11]. Additionally, the smaller FRC in children is maintained by physiological stenosis at the level of the cricoid and dynamically by tachypnea[12]. Thus, the pediatric FRC is not only small but also very unstable. Since sedatives, narcotics, and/or muscle relaxants often used in the PICU tend to diminish the FRC further, the risk of hypoxia increases correspondingly.
Based on these special features of child physiology, advanced warning of desaturation is needed. Though the ORI may provide the answer to this need, this device is not well distributed not only in Japan but also all over the world yet. The cases discussed here demonstrate that the ORI allowed us to re-oxygenate the patients before a desaturation event and minimize the severity of desaturation. Although further study is needed to validate our findings, this case report demonstrated the usefulness of the ORI in pediatric critical care.
The ORI can also be used in the pediatric general ward, emergency room, and imaging suite. In the imaging suite in particular, conscious sedation of children is often done. As described above, sedatives diminish the FRC and thereby increase the risk of hypoxia in children during imaging procedures. To ensure greater safety for sick children not only in the PICU but in pediatric medicine generally, using the ORI for advanced warning of desaturation is recommended.
NS, SO and OS managed the cases. SO measured ORI and analyzed data. NS, SO, and OS contributed to writing of the report. Consent to publication was obtained from the family. Publication was approved by the Institutional Review Board of Tokyo Metropolitan Children’s Medical Center. Authors thank Mr. James Robert Valera for his assistance with editing the manuscript.
The authors declare that they have no conflicts of interest regarding the content of this article.
Address correspondence to Dr. Naoki Shimizu.
Department of Pediatric Emergency & Critical Care Medicine,
Tokyo Metropolitan Children’s Medical Center, 2-8-29,
Musashidai, Fuchu, Tokyo 183-8561, Japan.
Phone: +81-42-300-5111. Fax: +81-42-312-8160.
E-mail: naoki_shimizu@mac.com
