




Chiba Medical J. 95E:11-16,2019
doi:10.20776/S03035476-95E-1-P11
[ Chiba Medical Society Award Review ]
Junichi Nakamura
Department of Orthopaedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670 .
(Received November 21, 2018, Accepted November 9, 2018, Published February 10, 2019.)
Total hip arthroplasty(THA) is a successful treatment for painful hip disorders. The direct anterior approach(DAA) in the supine position is a muscle-sparing technique that separates both the true intermuscular and internervous planes to reach the hip joint. The internervous plane consists of the femoral nerve and the superior gluteal nerve between the sartorius muscle and the tensor fascia lata in the superficial layer and between the rectus femoris muscle and the gluteus medius muscle in the deep layer respectively. A novel mobile traction table to facilitate DAA has been developed in collaboration between industry and academia. Furthermore, paradigm shifts in wound care have occurred, such as subcutaneous buried suture without skin suture, occlusive dressing, and drainless technique. Outcomes of traction DAA with ~As You Walk~ LECURⓇ are favorable in terms of shorter surgical time, less blood loss, less pain, and quicker recovery. Now another project for development of a novel total hip implant named“ MIRFY” has launched. In this regard, I would like to keep on evolving a new theory for patient’s happiness.
mobile traction table, total hip arthroplasty, direct anterior approach in the supine position
Total hip arthroplasty (THA) is a successful treatment for painful hip disorders such as osteoarthritis of the hip, osteonecrosis of the femoral head, rheumatoid arthritis, or hip fracture(Fig. 1). In Japan, the total number of joint replacement surgeries was about 220,000, and the total number of hip arthroplasties was about 130,000 in 2017(Yano Research Institute, https:// www.yano.co.jp/market_reports/C59109000, accessed 11 Nov 2018, in Japanese)(Fig. 2). Operative volume has doubled since 2001, and the market size is 60 billion yen. The direct anterior approach(DAA) in the supine position is a muscle-sparing technique that separates both the true intermuscular and internervous planes to reach the hip joint using the distal part of the Smith- Petersen approach[1]. This surgical approach has become of great interest over the last decade because of its quicker recovery and lower dislocation rates. A special traction table, initially proposed by Judet et al. [2], assists the surgeon by holding the leg in place and providing efficient exposure of the surgical field. Moreover, fluoroscopy guides implant alignment [3] (Fig. 3). However, DAA is still technically demanding. For these reasons, I started developing a novel mobile traction table to facilitate traction DAA.
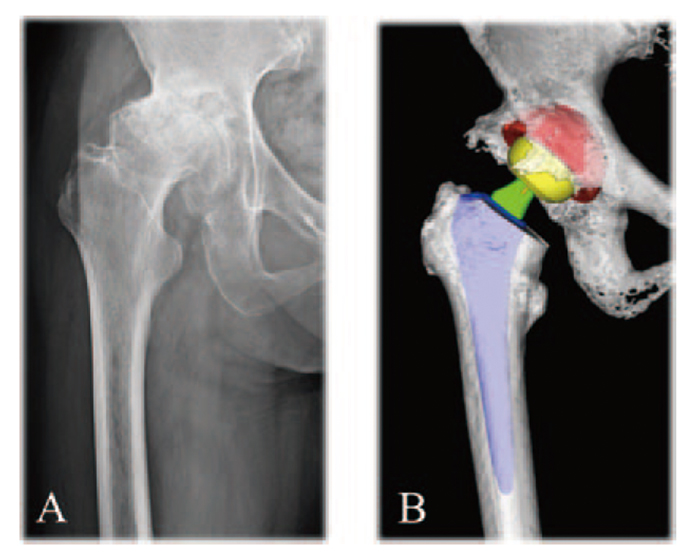
Fig. 1 Representative case of traction DAA
(A) This anteroposterior X-ray image shows osteoarthritis of the right hip.(B) Preoperative three dimensional computed tomography planning for THA: cup in red, head in yellow, neck in green, and stem in blue.
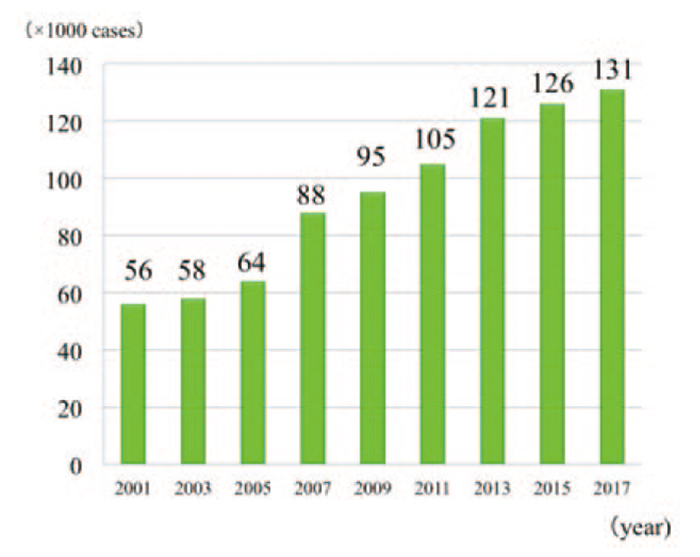
Fig. 2
Transitional change of number of hip joint replacement surgeries in Japan Operative volume has doubled since 2001.
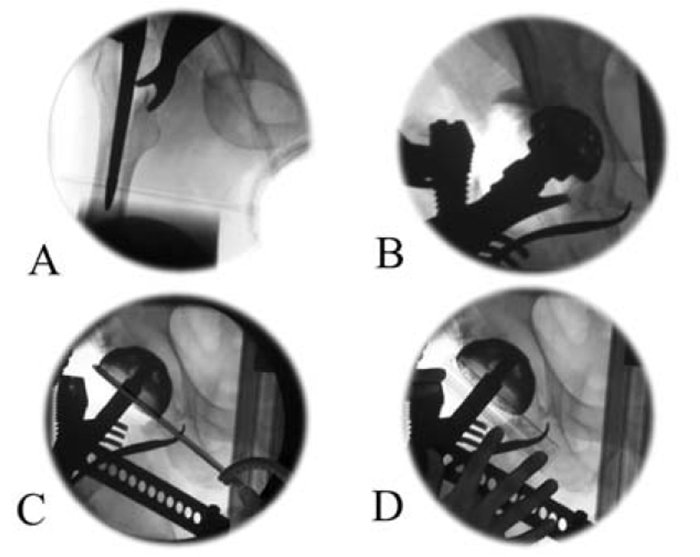
Fig. 3 Fluoroscopic monitoring
Intraoperative fluoroscopy monitors femoral rasping (A) and acetabular reaming(B). Cup alignment can be measured by goniometer for radiographic inclination(C) and by trigonometric function of minor axis/ major axis ratio for radiographic anteversion(D).
Around 2001, the treatment protocol for THA was as follows. A patient was hospitalized 4 weeks before surgery, blood for autotransfusion was taken twice(total 800 mL), preoperative general condition was examined including consultation to some specialists pro re nata and preoperative rehabilitation, and each case was discussed at conference before surgery. THA was a major surgery with one primary surgeon and three assistant doctors, with more than three hours of operative time and more than 1000 mL of intraoperative blood loss. THA was performed in the lateral decubitus position via the direct lateral approach, which split the iliotibial tract, gluteus medius muscle, gluteus minimus muscle, and vastus lateralis muscle (transgluteal approach). The skin incision was long, fitting the proverb“ great surgeon, big incision”(Fig. 4A). This approach had the advantage of wide exposure of the hip joint and ease of surgery, although it could cause abductor muscle weakness because of direct injury to the muscle and superior gluteal nerve denervation. A closed-suction drain was inserted to prevent hematoma with more than 1000 mL of postoperative blood loss. Staples or nylon thread was used for skin closure. Wound dressing was changed and sterilized every day. Bathing was permitted after wound healing and removal of the stitches about two weeks later. Discharge was approved 4 to 6 weeks afterwards, and thus total hospital stay was a few months.
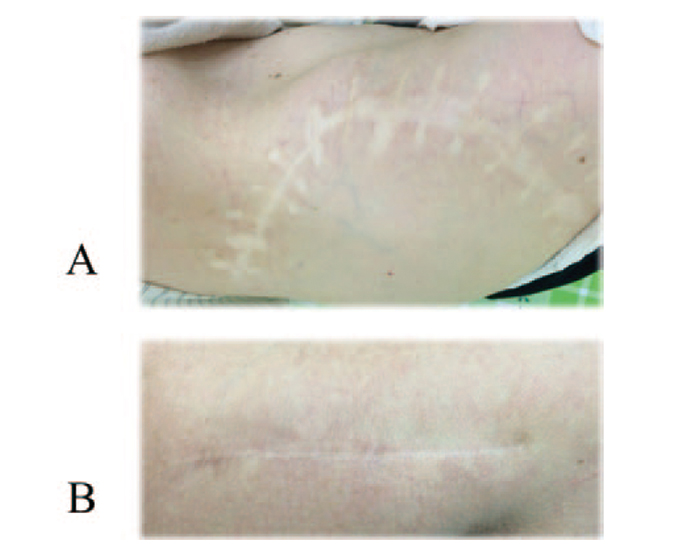
Fig. 4 Surgical scar around the hip
(A) A wound from 50 years ago is still conspicuous for stitch and incision marks.(B) Wound from subcutaneous buried suture without skin suture healed clear without stitch marks one year later.
In April 2010, I began to change the treatment protocol. First, subcutaneous buried suture without skin suture and occlusive dressing were introduced to make the scar inconspicuous(Fig. 4B). Patients could enjoy a shower from postoperative day 2, without wound dressing and sterilization until one week. Starting in July 2011, closed-suction drain was connected to a mobile cell saver to salvage postoperative blood loss, reducing preserved autotransfusion by roughly 1 unit(400 mL). In May 2012, traction DAA was introduced first in Japan. THA could now be performed twice a day and hospital stay could be reduced to three weeks. In July 2013, tranexamic acid was administered to reduce blood loss by the antiplasmin effect of hemostasis, and closedsuction drainage could be abandoned. In March 2015, THA was performed three times a day and hospital stay was reduced to two weeks. This meant a threefold increase in operative volume and a one-third decrease in hospital stay from 2001. Traction DAA has also contributed to reduction of the waiting period for surgery and medical cost. In January 2016, intraoperative local anesthesia and continuous subcutaneous injection of opioids took the place of epidural anesthesia due to decreased postoperative pain. This change has resulted in early rehabilitation and no risk of epidural hematoma.
Surgical site infection has been a great concern in postoperative management. The traditional idea was that the wound should be sutured tight, should be sterilized every day, and should be drained because microorganisms would infiltrate from the epidermis into the deep layer and proliferate in any hematoma. In 1962, Winter found in pigs that epithelization is retarded by the dry scab which normally covers a superficial wound, and if the formation of the scab is prevented, the rate of epithelization is markedly increased[4]. In the next year, Hinman suggested an occlusive dressing based on the evidence that in human skin wounds epidermal regeneration is faster when the wound surface is moist than when exposed to the air and dry[5]. However, occlusive dressing was not accepted among Japanese surgeons for long time. In 1990, Hadden and McFarlane first conducted a comparative study of closed-suction drainage versus no drainage in THA and demonstrated that the drainless technique has benefits of preventing retrograde infection and stabilizing hemodynamics[6]. Besides, all the bleeding was not always drained; for example if there was about 400 mL of drain blood loss and about 2000 mL of total blood loss, there remained about 1600 mL of blood under the skin[7]. Tranexamic acid, a synthetic analog of the amino acid lysine, was discovered in Japan[8]and has moved into the limelight again. It serves as an antifibrinolytic by reversibly binding plasminogen. As a result of this, closed-suction drainage became unnecessary. To prevent swelling and hematoma, a compressive bandage is necessary.
From May 15 to July 8 2014, an attitude survey was administered to identify response to occlusive dressing and drainless closure among orthopedic nurses. In three hospitals, 54 of 74 nurses(73%) answered the questionnaire. Mean experience was 8.9 years as a nurse and 4.6 years in the orthopedic department. For occlusive dressing, 92% of responses were favorable and 8% were unfavorable. Favorable opinions included that it was cost-effective, better for application of a novel wound dressing, and that there was clear wound healing; while opposite opinions included that the wound should be sterilized every day for patient feeling of security. For drainless closure, 35% of responses were favorable, 8% were unfavorable, and 57% were neither. Reasons for favorable opinion included early mobilization, no drain tube, no risk of retrograde infection, no foreign body sensation, reduced risk of hypovolemic shock, and no need to empty the drain bottle, while reasons for unfavorable opinions consisted of immeasurable postoperative bleeding and hematoma formation. For early shower, 79% were favorable and 21% were unfavorable. Favorable opinions included that patients felt refreshed, while unfavorable opinions included that bathing should be permitted only after the wound became painless or following removal of stitches. For subcutaneous buried suture without skin suture, 51% were favorable, 2% were unfavorable, and 47% were neither. Favorable opinions included that there was no need for painful removal of the stitches, better wound healing, reduced effort of medical staff, and no foreign body sensation, while unfavorable opinions included that there was risk of wound separation and that it was hard to judge the time of wound healing. This was a transition period for new concepts in wound dressing. Follow-up survey is of great interest to change the mind.
Traction DAA is performed with the patient in a supine position, utilized with a novel mobile traction table, ~As You Walk~ LECURE®[3](Fig. 5). This table can be set up with a standard orthopedic surgical table, and can hold the leg position in accordance with the surgeon’s preference. The leather boot is designed to fit the foot and ankle snugly with a double locking bandage mechanism to avoid slipping of the foot. From the superior anterior iliac spine, Heuter’s interval between the tensor fascia lata and sartorius muscle is palpated. The skin incision runs along the midline of the tensor fascia lata. The incision begins 3 cm proximal to the tip of the greater trochanter and 9 cm distal to the trochanter(12 cm long in total). With fluoroscopy, a vertical line passing through the tip of the greater trochanter is identified. The sheath of the tensor fascia lata is incised longitudinally in the direction of the muscle fibers. The muscle fibers of the tensor fascia lata are intentionally released laterally within the sheath using the surgeon’s index finger, and the deep fascia of the rectus femoris is identified as the tendinous fibers in white, muscle fibers as red, and fat tissue as yellow (tricolor sign). The femoral head is outlined using two narrow Homann retractors; one at the piriformis fossa and the other at the medial aspect of the femoral neck. The triangle of the anterior capsule is visualized; the medial line is the inferior iliofemoral ligament, the lateral line is the insertion of the vastus lateralis muscle and the capsule, and the superior line is the superior iliofemoral ligament. After capsulectomy, the upper outline of the cervicotrochanteric junction is visualized, then 45° of external rotation makes the lower outline clear, and mild traction causes subluxation. The osteotomy is performed in situ, perpendicular to the anterior inter-trochanteric plane. With traction, the osteotomy site is spontaneously opened and the femoral head can be easily removed. Femoral preparation is recommended before acetabular reaming(femoral first technique). Elevating the calcar femorale with a blunt hook, a sharp fork retractor is inserted into the posterolateral aspect of the greater trochanter. The ischiofemoral ligament and the superior iliofemoral ligament need to be detached until sufficient anterior mobilization of the greater trochanter is obtained. The pubofemoral ligament also needs to be detached to obtain sufficient lateral mobilization of the calcar. Hyperextension of 35°, relaxation and compression, and adduction of 10° are applied with the traction table. This relaxation technique prevents excessive stretch of the femoral nerve and also assists femoral exposure. A Z-shaped canal finder(Tanaka Ika, Tokyo, Japan) is an essential tool to identify the axis of the medullary canal and anteversion of the calcar. The entry point of the canal finder is the piriformis fossa; this is entered, avoiding flexion insertion or perforation of the femur. Femoral rasps are inserted sequentially. Acetabular reaming is performed with a straight holder, avoiding excessive reaming of the anterior and posterior walls of the acetabulum. Fluoroscopy intermittently monitors the height and the depth of the reaming, and the cup position(Fig. 3). Cup fixation is press-fit with two 20 mm screws. Reduction is performed by internal rotation and traction. Alignment of the implant and leg length discrepancy are confirmed with fluoroscopy. Anterior stability is examined by external rotation of 90° with mild traction.

Fig. 5 Trademark and design of a novel mobile traction table
From May 2012 to April 2014, 100 primary THAs in“ standard” patients without previous hip surgeries or severe deformity were consecutively divided into the first 50 cases and the second 50 cases using traction DAA. The implant survival rate was 99% at twoyear follow-up; one revision surgery was required for periprosthetic femoral fracture. Surgical complication possibly related by the traction table was 5%: there were 3 anterior dislocations, 1 periprosthetic femoral fracture, and 1 intraoperative perforation of the femoral rasping. Mean surgical time(72.0 minutes versus 82.5 minutes, p=0.027), rate of allogeneic blood transfusion(2% versus 24%, p=0.001), and cup alignment in the safe zone(100% versus 88%, p=0.027) were significantly improved in the second group compared to the first group. The preoperative JOA hip score was significantly improved at three months postoperatively, and continued to improve until 2 years postoperatively both in the first group and the second group(both p=0.001). At time of submission in November 2018, 537 patients had undergone traction DAA.
On November 1 2013, a contract for collaboration between industry(Surgical Alliance, Tokyo, Japan) and academia (Chiba University) was made and development of a novel traction table started. A fixedtype special traction table was too large and too expensive for those starting out conducting DAA, therefore a mobile and low-priced product was planned. Patent search revealed that in pre-existing traction tables, both traction and extension were carried out by one releasing operation. Thus, I invented the position adjustment unit with a grip unit which can carry out, by only one grip motion:(1) a first mode for fixing movement along the main frame and fixing adjustment of inclination of the support leg unit;(2) a second mode for releasing movement along the main frame and fixing adjustment of inclination of the support leg unit; and(3) a third mode for releasing movement along the main frame and releasing adjustment of inclination of the support leg unit. On April 11 2014, I went to Technology Licensing Organization(TLO) at Chiba University for an invention consultation. This invention was submitted to prior inspection on May 2, to the evaluation committee on May 7, and to the Japan Patent Office on July 29, 2014. This patent has been submitted for foreign application. Intellectual properties of ~As You Walk~ LECURE® are as follows: design right of accessory table on the traction frame to make the flat bed at start and end of general anesthesia; design right of transport carrier; registered trademark. LECURE was approved by Pharmaceuticals and Medical Devices Agency(PMDA) on September 12, 2014 and is now available for sale.
The market share of artificial joint implants is monopolized by foreign companies in Japan. There are several concerns in this situation. Academically, these imported products have been developed on the basis of skeletal structures of Europeans and Americans. Therefore, innovation of domestic implant is required to optimize the standards for Japanese skeletal structure. Economically, it is a serious trade deficit because no domestic companies export their products. In the industrial field, Japanese technology is highly appreciated in the world from electronics to automobile manufacturing. I believe that this medical device can be accepted as“ made in Japan” if it is high quality. Actually, our department has created total knee implants, such as Hi-Tech knee II by Emeritus Professor Hideshige Moriya and FINE knee by Emeritus Professor Toru Suguro[9]. In January 2016, another development project of a novel total hip implant named“ MIRFY” launched(Fig. 6). It will be approved by PMDA soon. Now I am challenging to establish Chiba Universityoriginated venture.

Fig. 6 Trademark and features of a novel total hip implant named“ MIRFY”
JN conceived of the study, participated in its design, and wrote the manuscript as the corresponding author. Written informed consent to publication was obtained from the patients.
I am grateful to the Chiba Medical Society. I thank all the investigators for collaborations on these works. I especially appreciate Mr. Yoshiyuki Kawasaki and Mr. Masato Tanimura (Surgical Alliance), Carter Technologies, Ishikawa Design, Masato Uchida(m-use), Mr. Keisuke Kohno(TLO, Chiba University), Mr. Masayoshi Takahashi (Kodama Patent Law Firm), and Emeritus Professor Kazuhisa Takahashi(Orthopaedic Surgery, Chiba University). I thank Professor Seiji Ohtori for critically reading this manuscript. This study was supported by collaboration between industry and academia, JSPS KAKENHI grant number 17K10954, grants from Mitsubishi Tanabe Pharma Corporation, Chiba Prefectural Federation of Small Business Association and Takeda Science Foundation.
JN has a financial relationship with Surgical Alliance for patents of the mobile traction table.
Address correspondence to Dr. Junichi Nakamura.
Department of Orthopaedic Surgery, Graduate School of
Medicine, Chiba University, 1-8-1, Inohana, Chuou-ku, Chiba
260-8670, Japan.
Phone: +81-43-226-2117. Fax: +81-43-226-2116.
E-mail: njonedr@chiba-u.jp
