




Chiba Medical J. 88E:9~12,2012
doi:10.20776/S03035476-88E-2-P9
[Review Article]
Robert Peter Gale1) and F. Owen Hoffman2)
1) Haematology Section, Department of Experimental Medicine, Division of Medicine, Imperial College, London,
UK W12 ONN.
2)SENES Oak Ridge, Inc., Center for Risk Analysis, 102 Donner Drive, Oak Ridge, TN 37830
(Received January 11, 2012)
Most people have only a few key questions regarding risk(s) associated with a past or possible future exposure to a potentially harmful substance. Foremost is the deceptively simple question: what is my risk? Other important issues are: How certain are you of the risk-estimate you are telling me? How does this risk compare to other risks in my life? Is my risk voluntary or involuntary? and What are my alternatives? People need this information for many reasons but especially for informed decision-making.
Effective communication of the risk of cancer in persons exposed to ionizing radiation is challenging. Conventional approaches of presenting cancer-risks are indirect and are typically point-estimates relying on units of dose or concentrations of a radioactive substance in the environment. Information given in this fashion is unlikely to inform most people; worse, it can be misleading. Communication of the potential health consequences of radiation exposure using units of dose also fails to consider that radiation-related cancer risk is highlydependent on the age at time of exposure remaining life-span, exposure to other cancer-causing agents(like smoking), co-morbid conditions and other variables not encompassed in the expression of dose.
The fundamental problem with relying on dose to express cancer-risk is that dose is only an intermediate quantity between exposure and risk. When dose is used to express risk it is typically compared with radiation benchmarks like regulatory dose-limits(ICRP, US EPA, NRC), doses associated with natural background radiations, doses from exposure to medical procedures (X-rays, CT-scans, radioisotope studies) and/or doses at the limits of a statistically significant detection of cancer risks observed in epidemiologic studies, like the Japanese A-bomb survivors. The implication is that if the estimated dose is below dose or concentration values used for these comparisons, there should be no cause for concern and that the risk at these dose levels is acceptable.
The limitations of using an estimate of dose or a level of radioactivity exposure or concentration as a surrogate for estimating risk are obvious, but is there a better way to express potential cancer-related hazards of radiation exposures to people?
Yes. Here are some alternatives:(1) total lifetime risk of cancer incidence(and/or cancer-related death) regardless of cause;(2) excess lifetime risk resulting only from additiona(l above baseline) radiation exposure; (3) future total and/or excess lifetime cancer-risk for persons exposed in the past(or who will be exposed soon) and who are currently free of cancer(radiationrelated or not); and(4) total and/or excess numbers of cancers anticipated in an exposed population over their lifetime. For persons previously-exposed to radiation who develop a potentially radiation-related cancer, risk can be translated into a person-specific assigned share sometimes called probability of causation.
All of these risk-estimates(and others) need to be quantified with regard to uncertainty which arises from several sources including:(1) uncertainty in subject-specific absorbed dose-estimates to each organ; (2) uncertainty in extrapolating dose-estimates into a risk-estimate to the individual or to a population; (3) statistical uncertainty in risk coefficients from epidemiological studies, like of the A-bomb survivors, for specific cancer-sites;(4) uncertainty in the model used to transfer risk-estimates from that seen in the A-bomb survivors to the US population for diseases with markedly-different baseline rates between the two populations(for example, breast and gastric cancers); (5) uncertainty in the model and coefficients used to extrapolate the dose-response observed at high doses and high dose-rates seen in the A-bomb survivors to settings where doses are lower and where exposure is prolonged over time and associated with either fractionated or chronic low-dose rates; and(6) uncertainty in extrapolating risks observed from the A-bomb survivors who were exposed primarily to an acute, high-energy gamma radiation to other types of radiation-exposures including alpha particles, neutrons, low energy beta particles(like tritium) and low energy photons(like X-rays).
Effective communication of cancer-risk to the public also requires a vital but volatile quantity: trust. Communicating cancer-risk assessments to people by dose-estimates and benchmarks without addressing the fundamental issue of cancer-risk associated with exposure may lead to a perception of censorship of risk information. Such perceptions of censorship diminish trust, which, once lost, is difficult if not impossible to regain.
People have bona fide concerns about radiationrelated cancer-risks and deserve direct, credible and intelligible answers. Information about risk should include uncertainty in risk-estimates that reflect current knowledge. We believe communication of a 95% uncertainty range or credibility interval is more informative than a single best estimate point-value. The upper limit of a 95% uncertainty range indicates of how high the risk might be whereas the lower limit represents a lower bound estimate of risk. If the upper limit is below a level of risk judged to be acceptable, the exposure may be regarded as low-priority and no action may be needed. However, if the lower limit is above a level of risk judged to be unacceptable, the exposure may be regarded as high-priority and may precipitate some form of action to reduce or eliminate exposure or even direct medical intervention.
Some scientists argue there is a threshold in the doseresponse relationship of radiation-exposure to cancerrisk such that there is no risk below a certain dose (usually somewhere between 50-200 mSv). However, the weight of evidence supporting this assumption is weak. Furthermore, even if the potential for a threshold effect were taken into account in cancer-risk estimation, this effect will have its’ greatest influence on the lower bound of a 95% uncertainty interval and only a minor influence on the upper bound estimate of risk. This is important because it is the upper bound of uncertainty in the estimate of cancer-risk that most concerns the public and which has the greatest implication for health protection. Moreover, arguing for a threshold-effect at low doses is difficult without a cogent biological explanation and without convincing evidence that exposure to background radiation is completely risk-free. As long as background radiation is assumed to be associated with some level of cancer-risk, any additional exposure to ionizing radiations, no matter how small, will increase the unavoidable risk associated with background radiation. Finally, arguing for a threshold effect, and therefore a radiation-dose associated with no cancer-risk, is likely to result in an erosion of public trust and should thus only be done when there is incontrovertible evidence to support this view. We think this level of evidence is lacking presently[1].
Cancer-risks of radiation-exposure should be estimated and communicated effectively. The challenge is to place this risk into context such that it can be compared to voluntary and involuntary cancer-risks in everyday life (naturally-occurring and environmental). Placing riskestimates into context helps people weigh the importance of a cancer-risk and decide whether a future exposure is acceptable. Equally important is the ability to compare cancer-risk(and uncertainty) with potential alternatives and with potential benefits(like having a CT-scan).
Information regarding the magnitude of a radiationrelated cancer-risk to other risks is important when communicating with the public. One useful approach is graphical comparisons in the form of risk-thermometers. Examples are Figure 1(Fig. 1) where we compare cancer-risks of different radiation-exposures and Figure 2(Fig. 2) where we compare cancer-risks of diverse involuntary exposures.
Other issues the public wants and needs to know to make informed decisions is not just the cancer-risk of radiation-exposure but: What type(s) of cancer we are talking about? How common is this type of cancer absent radiation-exposure? At what age is the cancer likely to occur? and What is my prognosis if I get a radiationrelated cancer? Consider, for example, non-melanoma skin cancers, thyroid cancer and lung cancer all of which are radiation-related cancers. Non-melanoma skin cancers are common without exposure to ionizing radiation, easily-treated and unlikely to be fatal. Getting one, especially at an older age, is unlikely to be extraordinarily upsetting to most people. Thyroid cancer is less common absent radiation-exposure, may require more extensive therapy, but is also unlikely to be fatal. Finally, lung cancer is relatively common like non-melanoma skin cancers, but therapy(if given) is most unpleasant, and survival after diagnosis is typically less than 6 months. The perception of the risk of lung cancer risk is also likely perceived differently by a young non-smoker than by an older person who has smoked most of his or her life. When we communicate radiation-related cancerrisk to the public we typically overlook these important considerations. Ways to improve on this situation are complex and continually being developed.
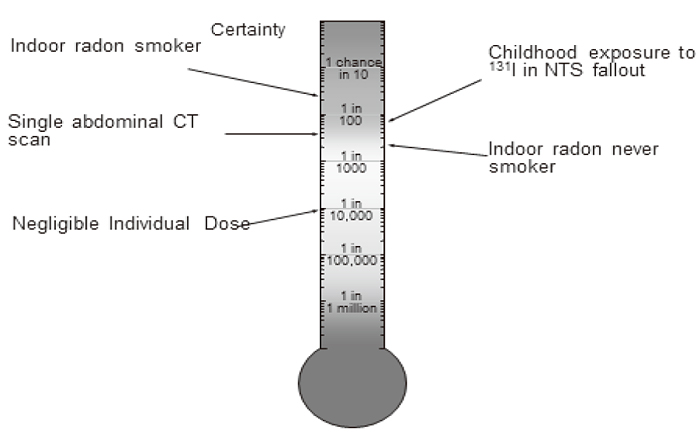
Fig. 1
Lifetime cancer-risk from exposure to radiation.
Original version with references at: www.senes.com/BeyondDoseAssessment/figure.1.htm. Indoor
radon levels of 46 Bq me-3; NTS fallout data
assume a female born in 1952 receiving a thyroid
dose of 0.1 Gy; CT scan in a 50 year old female;
negligible dose is 10 µSv ye-1 with a 70 y chronic
exposure.
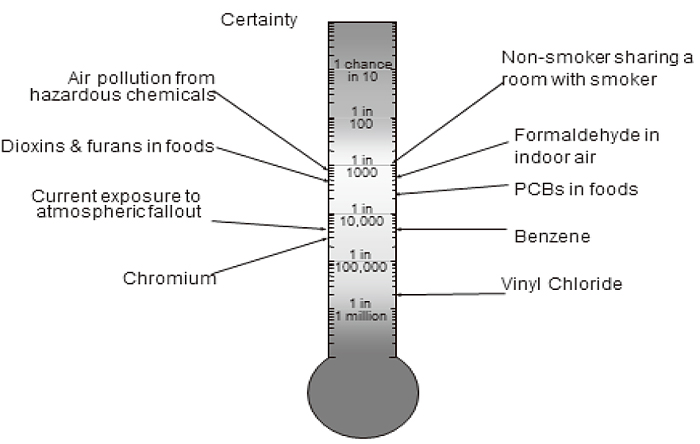
Fig. 2
Involuntary lifetime cancer-risk for several carcinogenic substances. Original color version and references at www.senes.com/BeyondDoseAssessment/figure.2.htm. www.senes.com/BeyondDoseAssessment/figure.1.htm. Air levels refer to outdoor air in California.
In summary, we believe direct assessment of cancerrisk from radiation-exposure including an expression of uncertainty rather than indirect assessment of cancerrisk using dose or the environmental concentration of a radioactive substance is more useful to informing the public of the potential importance of past, present or future radiation-exposures. It is especially important to acknowledge that the uncertainty in our risk estimates is based on our present knowledge and that this uncertainty may change as our state of knowledge improves. This approach will better inform the public and allow for more intelligent decision-making. It will also help build trust between scientists and the public, a step essential for effective communication.
Adopted from F. Owen Hoffman, David C. Kocher, and A. Iulian Apostoaei. 2011. Beyond dose assessment: using risk with full disclosure of uncertainty in public and scientific communication. Health Physics. 101: 591-600. We thank David C. Kocher and A. Iulian Apostoaei for their valuable contributions to our article.
1 )We recognize many epidemiological studies show no statistically-significant excess risk for cohorts exposed to high levels of background radiation( excluding the statistically-significant increased risk of lung cancer observed in epidemiological studies on residential exposures to radon decay products). However, these high background exposure studies cannot be used as direct evidence of the absence of cancer-risk without supporting mechanistic explanations. Precautionary interpretation of these studies, for purposes of health protection, is that cancer-risk associated with exposure to background radiation has not been detected at a high-level of statistical confidence even though the underlying cancer-risk is present. Evidence supporting the absence of exposurerelated cancer-risk at or near background dose levels should be considered when estimating the uncertainty in risk when exposures are below limits of epidemiological detection.
This working paper is directed towards members of the public, press and policy-makers; it is not intended as a detailed scientific review. Supporting references for our conclusions and opinions can be found in Hoffman FO, Kocher DC, Apostoaei IA. 2011. Beyond dose assessment: using risk with full disclosure of uncertainty in public and scientific communication. Health Physics. 101: 591-600 and are available from FOH and RPG. We thank our many colleagues whose detailed scientific studies underlie our views.
None. RPG is Visiting Professor of Haematology at Imperial College, on the medical staff of UCLA Ronald Reagan Medical Center, Los Angeles, CA and a part-time employee of Celgene Corp., Summit, NJ. F. Owen Hoffman is president of SENES Oak Ridge, Inc., Center for Risk Analysis. He is a distinguished emeritus member of the National Council on Radiation Protection and Measurements and a consultant to the United Nations Scientific Committee on the Effects of Atomic Radiation.
Address correspondence to Dr. Oh Hakumei. Branch of Chiba, Health Insurance Claims Review & Reimbursement Services, 2-1, Tonya-cho, Chuo-ku, Chiba 260-8521, Japan.
Phone: +81-43-241-9151. Fax: +81-43-248-1427.
E-mail: hakumei@chive.ocn.ne.jp
