




Chiba Medical J. 88E:55~58,2012
doi:10.20776/S03035476-88E-5-P55
[Case Report]
Takeo Furuya, Yoshikazu Tsuneizumi, Osamu Ikeda, Akihiko Okawa1)
Shunichi Kunishi, Jo Katsuragi, Mitsutoshi Ohta, Kazuhisa Takahashi1)
Masashi Yamazaki1) and Toshio Ohi
Department of Orthopaedic Surgery, Kamitsuga General Hospital, Tochigi 322-8550.
1) Department of Orthopedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
(Received August 21, 2012, Accepted August 30, 2012)
A 72-year-old man with a history of fall was admitted to our institute. Neurological testing demonstrated motor weakness of left upper limbs, showing grade 3/5 muscle strength for wrist and fingers. He had no sensory loss in his trunk or bilateral upper and lower extremities. Deep tendon reflexes were normal in both upper and lower extremities. Babinski signs were positive bilaterally. Radiologic examination showed fractures of cervical spine at the C3 and C6 levels which we classified as stage 3 compressive flexion fractures under the Allen classification system. Magnetic resonance imaging (MRI) showed a space-occupying lesion in the vertebral canal at the C3/4 level. We initially diagnosed the mass as a traumatic spinal subdural or subarachnoid hematoma. Diachronic MRI evaluation and enhanced-MRI and CT myelogram established the diagnosis of an intradural extramedullary tumor. To the best of our knowledge, no report has previously described finding an intradural extramedullary tumor incidentally during imaging studies of a traumatic injury at the same spinal level. Our experience suggests that the presence of atypical findings, such as oval shape, in a posttraumatic space-occupying spinal lesion should lead clinicians to consider the possibility that the lesion may be a tumor rather than a hematoma.
intradural extramedullary tumor, schwannoma, neurilemmoma, trauma, diagnosis, spinal hematoma
Intradural extramedullary tumors are generally slow growing and usually diagnosed only after they begin to cause symptoms such as local pain or neurological disturbances. However, such spinal cord tumors are sometimes discovered incidentally in association with trauma, screening magnetic resonance imaging (MRI). We now report a case of an intradural extramedullary tumor discovered incidentally during imaging studies of a traumatic injury at the same spinal level.
A 72-year-old man with a history of fall from stairs was admitted with incomplete left hemiplegia. He had a past medical history of intracerebral hemorrhage. He had no history of anticoagulant therapy. Routine blood tests, including coagulative parameters, were normal. Neurological testing demonstrated motor weakness of left upper limbs, showing grade 3/5 muscle strength, and left lower extremities showing grade 4/5 muscle strength. He had no sensory loss in his trunk or bilateral upper and lower extremities. Deep tendon reflexes were normal in both upper and lower extremities. Babinski signs were positive bilaterally. Radiologic examination detected swelling of the retropharyngeal space, along with a fracture line (called‘ fracture of the beak’) running from the anterior of the C3 vertebral body to the C3/4 intervertebral disk, plus a C4 spinous process fracture (Fig.1). A sagittal computed tomography (CT) image revealed the same type of fracture at C6 as seen at C3, along with spinous process fractures at C4, C7, Th1, and Th2 (Fig.1). We thus classified these fractures as stage 3 compressive flexion fractures under the Allen classification system. Midsagittal and axial MRI views showed a space-occupying lesion in the vertebral canal located on the middle to left side at the C3/4 level that showed isointensity with the spinal cord on T1-weighted images and high intensity on T2-weighted images (Fig.2). The mass had an oval shape and appeared to be located in the subdural or subarachnoid space. At a glance the mass looked ‘classic’ for an intradural tumor, we made an initial clinical diagnosis of either traumatic spinal subdural hematoma (SDH) or subarachnoid hematoma (SAH) because of the present history and the location of the mass. Because our patient had relatively minimal neurological symptoms, we initially chose a conservative approach in which we treated him by a halo-vest and Philadelphia color with the expectation that the mass would spontaneously regress over time. However, MRI one week after the injury and one month after the injury still showed no reduction in size and no signal change. MRI one month after the injury showed enhancement of the mass after intravenous administration of gadopentetate dimeglumine (Gd-DTPA) (Fig.3). A CT myelogram at this time revealed the presence of an intradural extramedullary tumor.
Having diagnosed this mass as an intradural extramedullary tumor, we proceeded to surgery because the tumor was causing extensive spinal cord compression. We performed a left hemilaminectomy of C2-6 with excising the tumor en-bloc under microscopy. The pathological diagnosis was schwannoma. No postsurgical neurological deficits resulted from the tumor excision. MRI after surgery showed no tumor recurrence and adequate decompression of the spinal cord. Follow-up examination six months after the surgery found that the patient had returned to his pre-injury activities of daily living level.
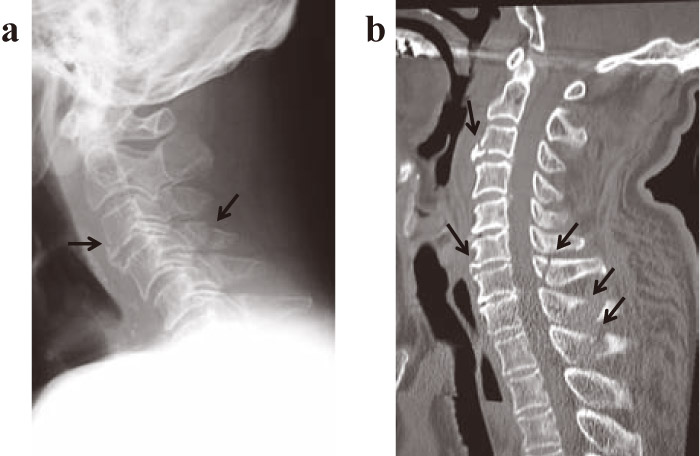
Fig.1
(a) X-p and (b) computed tomographic images of the cervical spine following spinal trauma in a 72-year-old man show injury to the C3 & C6 vertebral bodies which we classified as stage 3 compressive flexion fractures under the Allen classification system. Arrows denote the vertebral body and spinous process fractures.
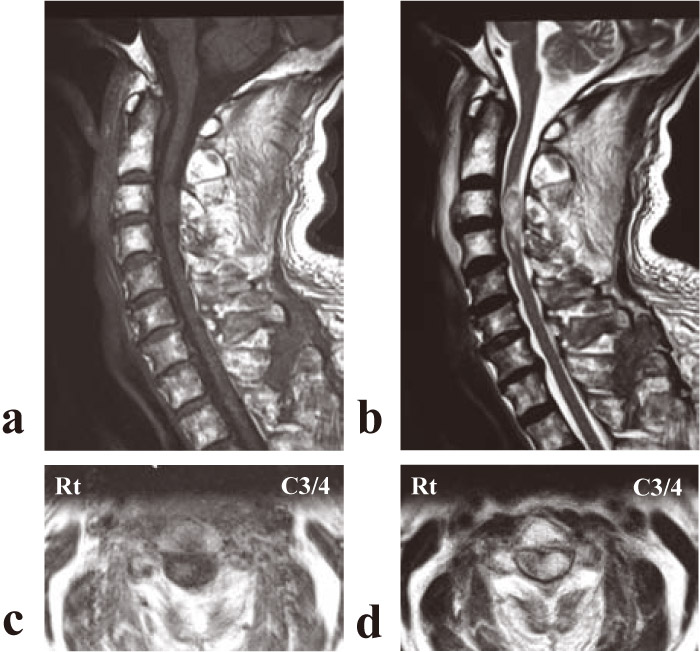
Fig.2
(a) T1-weighted midsagittal and (b) T2-weighted midsagittal of magnetic resonance imaging at the time of admission demonstrated a space-occupying lesion in the vertebral canal at the C3/4 level that showed an isointensity with the spinal cord on T1-weighted images and a high intensity on T2-weighted images. (c) T1-weighted axial and (d) T2-weighted axial views showed a round mass located on the left side of the spinal cord.
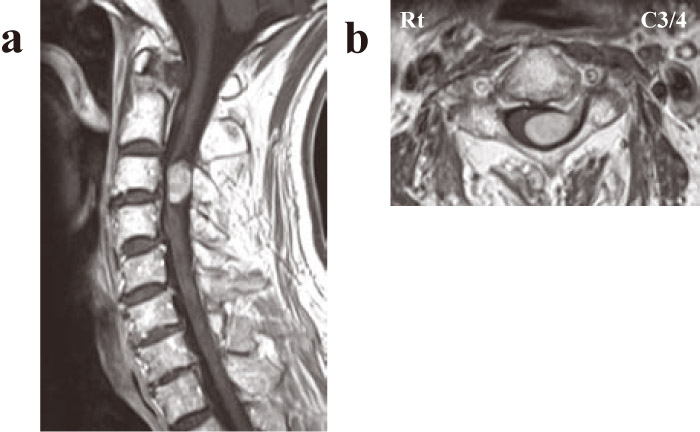
Fig.3
(a) T1-weighted midsagittal and (b) axial views of magnetic resonance imaging at the C3/4 level after injection of Gd-DTPA show definite enhancement of the mass.
Reviewing the imaging studies for our patient, we can identify several findings that helped with refuting the assumption that the mass lesion was a hematoma at an earlier period. First, the oval shape of the mass in the initial MR images was atypical for traumatic hematoma, as spinal SDH and spinal SAH usually spread longitudinally. Furthermore, the ongoing minimal degree of observed neurological impairment was discordant with the high level of spinal cord compression by the mass seen on MRI. That is, if the cord compression had occurred rapidly, as from a hematoma, more serious neurological symptoms should have soon developed in response. These two findings, then, should at least raise a suspicion that the mass was something other than a hematoma.
However, the strongest evidence against the mass being a hematoma developed over time, as subsequent MRI studies continued to show no change in the size or intensity the mass. Prior reports observed that traumatic hematomas do spontaneously resolve[1,2]. The lack of intensity change is particularly important in ruling out hematoma, as hemoglobin degrades to deoxyhemoglobin, methemoglobin, and hemosiderin over time, and each of these compounds have differing MRI absorption spectra. Thus the failure to observe intensity changes would imply that the mass was not a hematoma.
Spinal cord tumors are sometimes discovered after trauma[3-5]. In this case, we definitively ruled out hematoma by performing enhanced-MRI. Although we possibly might have diagnosed the tumor a bit earlier had we initially considered the possibility of a tumor and performed enhanced-MRI sooner, the clinical history of trauma implicated hematoma as the most likely cause at the outset. The diagnosis of tumor resulted largely from ongoing observation of neurological symptoms and repeated MRI evaluations over time.
To the best of our knowledge, this is the first report that describes the incidental discovery of an intradural extramedullary tumor during imaging studies of a traumatic injury at the same spinal level. In this case, we arrived at the correct diagnosis through diachronic MRI evaluation and enhanced-MRI, following which we successfully excised the tumor. Our experience with this patient leads us to conclude that enhanced-MRI can be a useful tool for diagnosing spinal tumors even in trauma cases. Furthermore, the differential diagnosis of spaceoccupying posttraumatic spinal lesions should include at least the possibility of a tumor as well as hematoma.
Address correspondence to Dr. Takeo Furuya.
Department of Orthopedic Surgery, Graduate School of Medicine, Chiba University, 1-8-1 Inohana, Chuo-ku, Chiba 260-8670, Japan.
Phone: +81-43-226-2117. Fax: +81-43-226-2116.
E-mail: takeo1225@snow.plala.or.jp
