




Chiba Medical J. 89E:1~7,2013
doi:10.20776/S03035476-89E-1-P1
[Original Paper]
Kento Nawata, Yasuhiro Oikawa, Takana Koshi, Sumihisa Orita
Kazuyo Yamauchi, Yasuchika Aoki, Tetsuhiro Ishikawa, Masayuki Miyagi
Hiroto Kamoda, Miyako Suzuki, Gou Kubota, Yoshihiro Sakuma
Kazuhide Inage, Takeshi Sainoh, Junichi Nakamura, Masashi Takaso
Gen Inoue, Tomoaki Toyone, Kazuhisa Takahashi and Seiji Ohtori
Department of Orthopedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
(Received January 4, 2013, Accepted January 25, 2013)
Purpose: Vertebral compression fracture(VCF) is one of the main adverse clinical consequences of osteoporosis. Pain relief is the principal objective when treating VCFs in elderly people. Balloon kyphoplasty(BKP) using bone cement is a minimally invasive approach for vertebral augmentation available for the management of symptomatic VCFs. However, to our knowledge, clinical investigation of BKP for VCFs in Japan has not yet been reported in the English literature. The purpose of the current study was to examine the clinical efficacy of BKP for VCFs in Japanese patients with osteoporosis.
Methods: We evaluated 5 patients with VCFs as a result of osteoporosis. Fracture levels were T12 in one patient and L1 in 4 patients. Conservative treatment for pain was not effective in any patient over 3 months. BKP was performed under general anesthesia. Results: BKP for VCFs was effective for low back pain during 12 months compared with that before surgery. The kyphotic angle at the fracture site significantly improved immediately after surgery and was maintained for 12 months. However, one patient showed adjacent VCF 4 months after surgery. We added BKP at the adjacent VCF.
Conclusions: We evaluated the efficacy of BKP for VCFs with osteoporosis. Pain reduction and maintenance of reduction of kyphotic angle were obtained after BKP surgery. However, we need to be aware of its complications.
Balloon kyphoplasty, vertebral compression fractures, osteoporosis, pain
Vertebral compression fracture(VCF) is one of the main adverse clinical consequences of osteoporosis. The age standardized incidence of morphometric fracture is 10.7/1,000 person years(pyr) in women and 5.7/1,000 pyr in men[1]. The age-standardized incidence of vertebral fracture as assessed qualitatively by radiologists is broadly similar-12.1/1,000 pyr and 6.8/1,000 pyr, respectively[1]. The incidence increased markedly with age in both men and women[1]. Medicare accounts for more than 80% of insurance for treatment of VCFs[2]. There has been a staggering increase in the number of vertebral augmentation procedures performed between 1993 and 2004 in the United States[2]. The“national bill” for inpatient hospitalizations for VCFs totaled $1.3 billion in 2004[2].
Conservative treatment for VCFs, without surgery has been the criterion standard. However, low back pain and disability because of VCFs are often serious problems for elderly patients[3]. The number of vertebral deformities is strongly associated with kyphosis, difficulties in activities of daily living, poor performance, and low back pain[3].
Pain relief is the principal objective when treating VCFs in elderly people. Vertebroplasty and balloon kyphoplasty(BKP) are minimally invasive approaches for vertebral augmentation available for the management of symptomatic VCFs[4]. The insertion of a bone cement(polymethylmethacrylate) or a bone substitute (calcium phosphate) into the vertebra is thought to stabilize the fracture, relieve pain, and in some cases of recent mobile fractures, restore lost vertebral height[4]. Vertebroplasty involves the percutaneous injection of cement, such as polymethylmethacrylate, directly into the cancellous bone of a vertebral body with the goal of alleviating pain associated with a vertebral compression fracture and preventing further loss of vertebral body height or progression of kyphotic deformity[5]. BKP was introduced later as a modification of vertebroplasty in which a balloon tamp is inflated in the vertebral body to compress the cancellous bone and create a cavity. Theoretically, the cavity allows the cement to be injected under less pressure and minimizes extravasation[5]. Previous investigators have reported the benefits and risks associated with vertebroplasty and BKP. Both vertebroplasty and BKP provide significant improvement in low back pain scores[6,7]. However, vertebroplasty has statistically greater risk of cement leakage and new fracture compared with BKP[6,7].
Last year, BKP was approved as a treatment for VCFs in the Japan. However, to our knowledge, clinical investigation of BKP for VCFs has not yet been reported in the English literature. The purpose of the current study was to examine the clinical efficacy of BKP for VCFs in Japanese patients with osteoporosis.
The ethics committee of our institution approved the protocol for the human procedures used in this study. Informed written consent was obtained from each subject.
Patients
We evaluated 5 patients in our University hospital who had treatment for low back pain with thoracic and lumbar VCFs at our hospital between January 2011 and April 2011. Patients had low back pain, continuing for at least 3 months. Patients were diagnosed with thoracic and lumbar VCFs on X-ray and magnetic resonance imaging, and computed tomography. Patients who had previously undergone spinal surgery were excluded. We also excluded spinal tumor, infection, and acute vertebral burst fractures of the thoracic and lumbar spine. Finally, 5 patients with osteoporosis aged 62-83 years (mean ± SD: 80.0 ± 6.9 years) were examined. All of them were diagnosed as having osteoporosis based on Japanese criteria[8]. Bone mineral density(BMD) in the lumbar spine was examined before surgery. Details of the patients’ backgrounds are shown in Table 1 (Table 1).
All patients underwent BKP surgery at the level of their VCFs (Fig.1A). We did not use other osteoconductive products for treatment of fractures.
Administration of risedronate
Patients were administered a bisphosphonate (weekly oral administration of 17.5 mg risedronate, Eisai, Tokyo, Japan) for osteoporosis before and after surgery. Patients were allowed to use nonsteroidal antiinflammatory drugs for pain control before and after surgery.
Radiographic and clinical evaluation
Radiography was used to evaluate bone stability. Profile views of X-ray images before, and 1 week, 3, 6, 9, and 12 months after surgery were evaluated. Evaluation of the kyphotic angle was blinded and conducted by 3 surgeons (Fig.1B).
Table 1
Demographic Characteristics
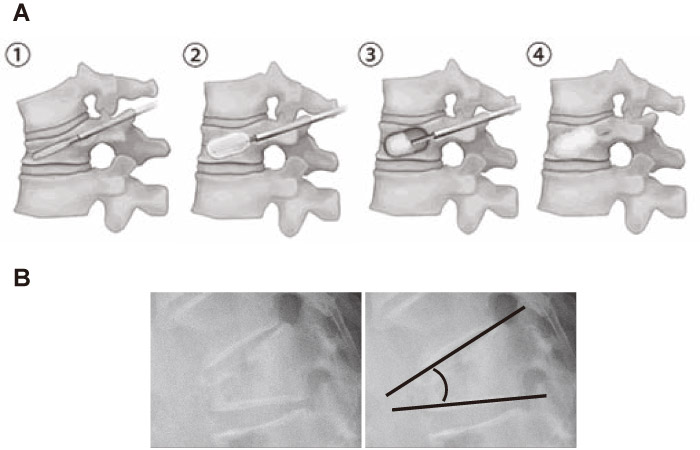
Fig. 1
A: BKP method.
1, Balloon tamp is inserted through the pedicle.
2, Balloon tamp is inflated in the vertebral body to compress the cancellous bone and create a cavity.
3, Cement is used to fill the cavity.
4, Cement fully fills the cavity.
B: Measurement of kyphotic angle.
Pain score
To evaluate change in low back pain, the visual analogue scale(VAS) score(0, no pain; 10, worst pain) for low back pain was recorded before surgery, 1 week after surgery, and 12 months after surgery, and compared.
Adverse events
All adverse events were reported together with an assessment of their severity and the investigator’s opinion of their relationship to the treatment with each procedure.
Statistical analyses
A Kruskal-Wallis test was used to compare pain scale data before and after surgery, a one-way ANOVA with post hoc comparisons for follow-up data, and Fisher’s test was used for dichotomous or categorical variables. P<0.05 was considered statistically significant.
Table 1 (Table 1) shows demographic characteristics of the patients before surgery. Average BMD(YAM) was 65 ± 5%, and they showed less than 70%. The level of fracture was T12 in one patient and L1 in 4 patients. There were no drop out patients during the follow-up period.
Figure 2 (Fig.2) shows VCF at the L1 level in an 81-year-old woman with low back pain. The patient underwent BKP, and her kyphotic angle improved and low back pain significantly decreased after surgery.
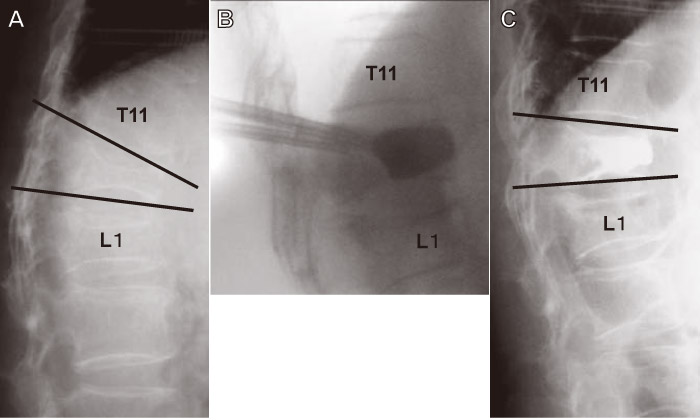
Fig. 2
X-ray films before(A), during surgery(B), and 12 months after BKP surgery in an 82-year-old woman with osteoporotic VCF. The kyphotic angle improved after surgery.
Table 2 (Table 2) shows a summary of low back pain score before and after surgery. VAS score significantly improved 1 week after surgery compared with that before surgery in 5 patients(P<0.05; Table 2 (Table 2)). VAS score at final follow-up(12 months after surgery) for patients also significantly improved compared with that before surgery(P<0.05; Table 2 (Table 2)).
Table 3 (Table 3) shows a summary of the kyphotic angles before and after surgery. The average kyphotic angle was 24 ± 5° before surgery; however, this angle significantly improved 1 week after surgery(14 ± 3°)(P<0.05). The average kyphotic angle was maintained 12 months after surgery(16 ± 4°) and was significantly better compared with that before surgery(P<0.05).
Table.2
Low back scores before and after surgery

Table.3
Kyphotic angle before and after surgery

Figure 3 (Fig.3) shows complications after surgery. A 76-year-old man underwent BKP surgery at the L1 level; however, an adjacent VCF occurred at the T12 level. Additional BKP surgery was performed at the T12 level; the patient showed no low back pain 12 months after first surgery.
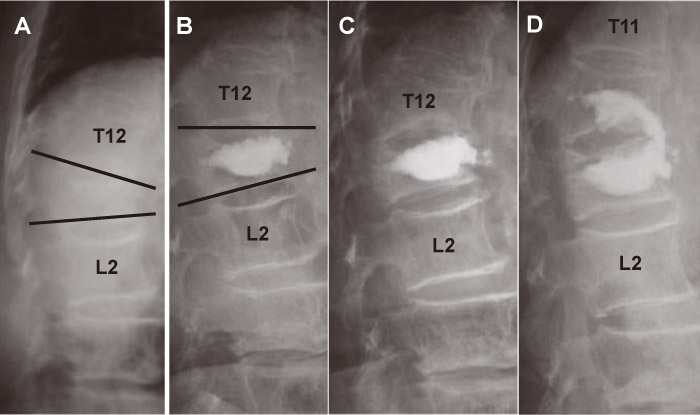
Fig. 3
X-ray films before(A), 1 week after surgery(B), and 4 months after BKP surgery, and 12 months after first BKP surgery in a 76-year-old man with osteoporotic VCF. X-ray films show an upper adjacent VCF(T12) 4 months after BKP surgery(C). Additional BKP was performed at the T12 level.
In the current study, we showed that BKP for VCFs is effective for low back pain and improvement of kyphotic angle. However, we should aware of its effectiveness and complications. One patient showed an adjacent VCF 4 months after surgery.
Several authors have reported the cost and effectiveness of BKP surgery for the pain of VCF [9,10]. Randomized controlled studies comparing conservative and BKP treatment for VCFs have been reported [9]. Three hundred randomly-assigned patients with acute VCFs were divided into BKP treatment(n=149) or nonsurgical care(n=151). This randomized controlled trial showed that in patients with acute, painful, vertebral fractures, BKP improved quality of life, function, mobility, and pain more rapidly than nonsurgical management, with significant differences in improvement between the groups [9]. Svedbom et al. used economic analysis, which was performed from a health care perspective, and used quality-adjusted life years for measuring health effects as recommended by the National Institute for Health and Clinical Excellence; they reported the cost-effectiveness of BKP compared with nonsurgical management for the treatment of hospitalized VCFs in the UK[10].
Several authors have reported the effectiveness of radiographic features for assessing the outcomes of BKP [11,12]. In 2005, Kasperk et al. published findings at three and six months of follow-up and Grafe et al. published findings at 12 months of follow-up comparing BKP with optimal medical management in 60 patients [11,12]. Sixty patients with primary osteoporosis and painful VCFs presenting for >12 months were includedin the prospective, nonrandomized controlled study [11,12]. BKP increased midline vertebral height of the treated vertebral bodies by 12.1%, whereas in the control group, vertebral height decreased by 8.2%(P= 0.001)[11,12]. The current study shows the efficacy of BKP on pain and radiographic features in Japanese patients, and this was consistent with previous reports.
By contrast, Boonen et al. reported limitations of BKP. Adults with one to three vertebral fractures were randomized within 3 months from onset of pain to undergo BKP(n=149) or nonsurgical therapy(n=151)[13]. Compared with nonsurgical management, BKP rapidly reduces pain and improves function, disability, and quality of life without increasing the risk of additional vertebral fractures [13]. The differences from nonsurgical management are statistically significant when averaged across 24 months; however, most outcomes were not statistically different at 24 months [13]. In this regard, we need to collect longer follow-up data using a larger population in Japan.
In the current study, we experienced adjacent VCF at the T12 level 4 months after BKP surgery. Additional BKP surgery was performed at the T12 level. In a previous report, the comprehensive metaanalysis by Lee et al. summarized all published BKP complications. Cement leakages occurred in 14% of all cases, but only 0.01% were symptomatic. New vertebral fractures occurred in 17% [14]. Taylor et al. reported that 189(9.0%) cement leakages were found in 2,239 vertebrae that underwent BKP [15]. One leak(0.001%) was reported to be symptomatic. A total of 171 new or incident fractures were reported in 1,151 patients across 16 studies, 110(64%) of which occurred in the vertebrae adjacent to the procedure [15]. The overall rate of mortality of 3.2% reflects both the age of patients undergoing BKP, as well as the inclusion of patients with cancer. The perioperative mortality rate was 0.01% [15]. We advise taking these adverse events into consideration before, during, and after BKP surgery.
The current study has some limitations. First, it is a small-sized study, and the number of patients was restricted. Second, the follow-up period was within one year. Clearly, further studies with larger numbers of patients for a longer time are required to improve our data.
In conclusion, the current study found that pain reduction and maintenance of improvement of kyphotic angle were obtained for 1 year after BKP surgery for VCFs in patients with osteoporosis. We believe that BKP is an effective treatment for VCFs in patients with osteoporosis.
The authors have no acknowledgments.
The authors did not receive any financial funding for data collection, analysis, or writing of the manuscript.
The authors did not receive and will not receive any benefits or funding from any commercial party related directly or indirectly to the subject of this article.
Address correspondence to Dr. Seiji Ohtori.
Department of Orthopedic Surgery, Graduate School of Medicine, Chiba University, 1-8-1 Inohana, Chuo-ku, Chiba 260-8670, Japan.
Tel.+81-43-226-2117. Fax. +81-43-226-2116.
E-mail: sohtori@faculty.chiba-u.jp
