




Chiba Medical J. 89E:35~40,2013
doi:10.20776/S03035476-89E-6-P35
[Original Paper]
Kazuhiro Nogawa1), Kouichi Sakata1), Mitsuhiro Oishi1)
Kumihiko Tanaka1) and Yasushi Suwazono1,2)
1) Department of Occupational and Environmental Medicine, Graduate School of Medicine, Chiba University, Chiba 260-8670.
2) Center for Preventive Medical Science, Chiba University, Chiba 260-0856.
(Received June 4, 2013, Accepted June 18, 2013)
Objectives: This study was undertaken to determine whether a causative relationship exists between the development of hypo high-density-lipoprotein (HDL) cholesterolemia and increased highsensitivity C-reactive protein (HsCRP).
Methods: The target population comprised 6,985 male workers at a Japanese steel company. The prospective cohort study was performed over a 5-year period, and annual health screening information was analyzed by a pooled logistic-regression method.
Results: A significant relationship between the development of hypo HDL cholesterolemia and increased HsCRP was observed, after adjusting for confounding factors such as various blood chemistry parameters and lifestyle factors (smoking, drinking, exercise, meals), job schedule type and job stress. The odds ratio of a 1.5-fold increase in HsCRP was 1.05 (95%CI: 1.03-1.08).
Conclusions: The results suggested that an increase of HsCRP is associated with the development of hypo-HDL-cholesterolemia.
High-sensitive C-reactive protein, High density lipoprotein Cholesterol, Workload, Lipid metabolism, Dyslipidemia, Cohort study
A number of epidemiological and clinical studies have shown a relation between plasma high-densitylipoprotein (HDL) cholesterol level and atherosclerotic diseases[1-5]. This makes it important to identify factors that promote decreased HDL levels to help prevent atherosclerotic diseases. On the other hand, high-sensitive C-reactive protein (HsCRP) is a protein marker of acute phase and systemic inflammation. A significant relationship has also been demonstrated between HsCRP and atherosclerotic diseases[6-8].
Many studies are available on the relationship between HDL levels and HsCRP level, most of which have demonstrated a negative association between HsCRP and HDL[9-13]. Therefore, it is generally considered that high levels of HsCRP promote low levels of HDL.
However, almost all of the previous studies showing a negative association between HsCRP and HDL were cross-sectional in nature.
In terms of effect of inflammation on low HDL cholesterol level, Zuliani et al. [14] indicated that interleukin 6, together with other cytokines, might influence HDL cholesterol levels by modifying the activity of the triglycerides lipases. It has been shown that pro-inflammatory cytokines inhibit the activity of lipoprotein lipase[14,15], and enhance the lipolytic activity of endothelial lipase[14,16], Both these actions have been associated with low HDL-C levels during acute or chronic inflammatory states[14]. On the other hand, HDL cholesterol may decrease CRP level by its anti-inflammatory effects including inhibition of cytokine-induced adhesion molecule expression in endothelial cells, inhibition of monocyte adhesion to the endothelium, inhibition of monocyte activation resulting in an inhibition of proinflammatory cytokines and chemokine production, reduction of neutrophil activation and inhibition of neutrophil infiltration in the arterial wall[17].
Therefore, from the epidemiological point of view, cohort studies are necessary to demonstrate any causative relationship between HsCRP and HDL, but to our knowledge no such cohort studies have been published.
This promoted us to examine the relationship between levels of HsCRP and HDL by means of a cohort study and to clarify whether a causative relationship exists between them or not.
This prospective cohort study included observations made over a 5-year period from 2005 to 2010. A total of 6,985 subjects out of a possible 9,546 male workers at a Japanese steel company were enrolled. The following individuals were excluded from this study: those who did not receive a health examination in the subsequent year (869 men), those for whom the measurement of HDL was missing in the subsequent year (596 men), those who had a history of collagen disease (48 men), those who had been diagnosed with hypo-HDLcholesterolemia based on the criteria in the present study (955 men), and those with any missing data in the year of entry (93 men).
The health examinations were carried out between 09:00 and 15:00 throughout the study period, with none of the measurements taken within 30 minutes of a meal or heavy physical activity. Occupational physicians carried out the examination and verified the medical history. The endpoints in the study were defined as follows: A value of HDL cholesterol less than 40mg/ dl, and/or starting to take an antilipotropic drug. We used the cut-off value of HDL cholesterol of 40mg/ dl because the Japan Atherosclerosis Society defines hypo-HDL-cholesterolemia as an HDL cholesterol of less than 40mg/dL[18]. The annual health examination contained the serum HsCRP level, which was measured by alatex turbidimetric immunoassay method[19].
The minimum detectable concentration and interassay coefficient of variation for HsCRP were 0.02 mg/dL and 2.43%, respectively. Age, body mass index (BMI), systolic blood pressure, diastolic blood pressure, HDL cholesterol, HbA1c, aspartate aminotransferase (AST), creatinine and uric acid were measured during the study, with alcohol consumption, soft drink consumption, and smoking and exercise habits serving as covariates in the analyses. All covariates were updated whenever the annual health examination was carried out. We calculated the value of mean arterial pressure (MAP) using the equation (diastolic blood pressure × 2 + systolic blood pressure)/3[20]. Type of job schedules, habitual exercise, cooking by oneself or other, softdrink consumption, smoking habits and snacking between meals were recorded using self-administered questionnaires during the health examination. Type of job schedule was categorized as daytime, three-shift work, two-shift work, or other, and in the same way, smoking habits as non-smoker or smoker; habitual exercise as none, 1-2 times/ month, 1-2 times/ week, 3-4 times/ week or ≧5 times/ week; meals as cooked by oneself, cooked by family member, eating out or catering, eating in a dormitory or other; soft-drink consumption as rare, occasional or frequent; and snacking between meals as rare, occasional or frequent.
The volume of alcohol in each type of alcoholic beverage was calculated using the unit‘ gou’. In Japan ‘gou’ is the most common unit used to measure alcohol consumption: 1 gou (180 mL) of Japanese sake (rice wine) contains approximately 22 g of ethanol, and is equivalent to 500 mL of beer, 60 mL of whiskey, 180 mL of wine and 110 mL of shochu (distilled spirits).
This unit was used in the questionnaire as it is easily comprehensible by the general Japanese population to determine the amount of alcohol beverages consumed.
Weekly alcohol intake was estimated by multiplying quantity by frequency. Job-related stress factors were evaluated by the Brief Job Stress Questionnaire (BSJQ) [21] and were included as covariates.
The study protocol was approved by the Ethics Review Board of the Graduate School of Medicine, Chiba University.
A pooled logistic-regression analysis was used to examine the relationship between HsCRP and the development of hypo-HDL-cholesterolemia. The HsCRP, HDL HbA1c, AST, creatinine and uric acid were log-transformed. In a pooled logistic-regression analysis, each examination interval of 1 year was treated as a mini follow-up study. The parameters obtained at the beginning of each 1-year follow-up were linked to the development of hypo-HDL-cholesterolemia at the end of the follow-up. Then, these 1-year followups were pooled and the relationships between parameters obtained in the development of hypo- HDL-cholesterolemia were analyzed using a logisticregression model [22]. The analyses were performed using IBM SPSS 19J statistical software (IBM Business Analytics, Tokyo, Japan). P values <0.05 were considered statistically significant.
Characteristics of the subjects for hypo-HDLcholesterolemia at study entry year are presented in Table 1(Table 1). The mean age was 44.6 years. The geometric mean (GM) of HsCRP was 0.05 mg/dL and the GM of HDL cholesterol was 54.9 mg/dL. Table 2 (Table 2) shows the number of person-years studied and incidence rate.
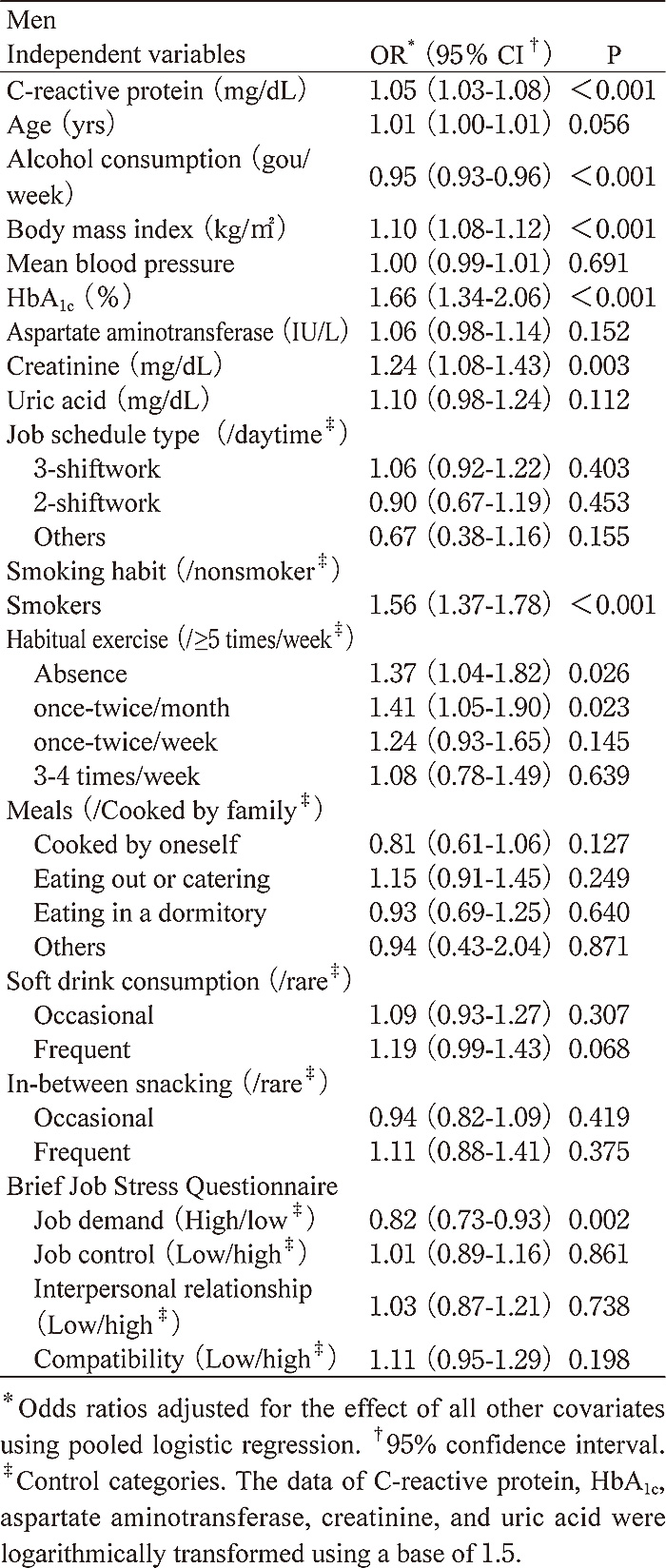
The number of subjects who developed hypo HDLcholesterolemia was 1,156 and the incidence rate was 16.5%. Table 3 (Table 3) shows the odds ratios (OR) and 95% confidence intervals (CI) for the development of hypo-HDL-cholesterolemia. The data of HsCRP, HbA1c, aspartate aminotransferase, creatinine, and uric acid were logarithmically transformed using a base of 1.5. This shows that increased serum HsCRP was associated with hypo-HDL-cholesterolemia. The OR of a 1.5-fold increase in HsCRP for the development of hypo-HDL-cholesterolemia was 1.05 (95%CI: 1.03- 1.08). BMI [OR (95%CI): 1.10 (1.08-1.12)], HbA1c [OR (95%CI): 1.66 (1.34-2.06)], creatinine level [OR (95%CI): 1.24 (1.08-1.43)], smoking habit [OR (95%CI): 1.56 (1.37-1.78)] and little habitual exercise (0 times [OR (95%CI): 1.37 (1.04-1.82)] or once-twice/month [OR (95%CI): 1.41 (1.05- 1.90)]) had associations with the development of hypo- HDL-cholesterolemia, while alcohol consumption [OR (95%CI): 0.95 (0.93-0.96)] and job demand [OR (95%CI): 0.82 (0.73-0.93)] had negative associations.
Table 1
Characteristics of subjects for hypo-HDLcholesterolemia at study entry year in men
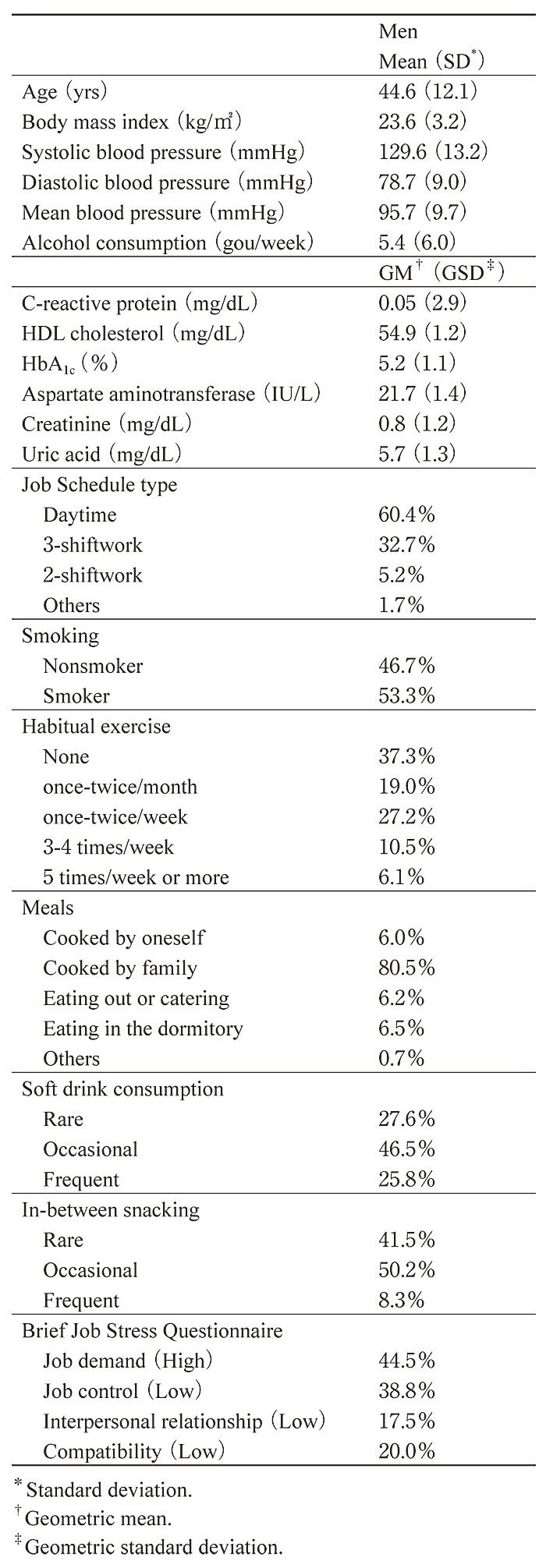
Table 2
Number of person-years studied and incidence rate.
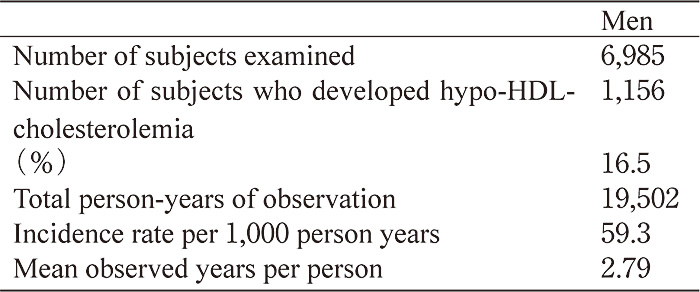
Table 3
Odds ratios and 95% confidence intervals for the development of hypo-HDL-cholesterolemia in men.
This study demonstrated that high HsCRP had an effect on the development of hypo-HDL-cholesterolemia in Japanese male workers even after adjusting for potential confounders. To our knowledge, few studies have demonstrated a relationship between high HsCRP and the development of hypo-HDL-cholesterolemia, using a cohort method. Salient points of this study are as follows. First, it used data from a large number of persons (6,985 men). The data included blood chemical data, data on diverse lifestyle factors such as smoking, drinking, exercise, meals, and job schedule type and job stress. Numerous confounding factors were included and adjusted for in defining the relationship between HsCRP and the development of hypo-HDL-cholesterolemia.
Second, pooled logistic regression analysis was used for analyzing the relationship between HsCRP and the development of hypo-HDL-cholesterolemia. The annual health examination was performed from 2005 to 2010 and all of the data from this 5-year period could be used and evaluated by this analytical method. A pooled logistic-regression analysis is appropriate and very effective for analysis of the data from multiple years and can adjust for covariates as well. In addition, this study excluded participants with chronic inflammatory disease and hypo-HDL-cholesterolemia at the start.
On the basis of these findings, it can be said that high HsCRP level promotes hypo-HDL-cholesterolemia.
The mechanism underlying this finding is unclear, however, and will require further study.
In addition, this study demonstrated that BMI, HbA1c, creatinine level, smoking habit and little habitual exercise (0 times or once-twice/month) were similarly associated with the development of hypo-HDL-cholesterolemia. In the present study, the ORs for other significant factors were generally larger than that of HsCRP. Therefore, the impact of HsCRP on the development of hypo-HDL-cholesterolemia may be limited compared to other significant factors such as obesity or lifestyle factors. On the other hand, after the standardization of significant ORs based on the geometric standard deviation of each biochemical measurements, the ORs were estimated to be 1.15, 1.15 and 1.09 for HsCRP, HbA1c and creatinine, respectively. Therefore, we consider that the relative impact of HsCRP were comparable to those for HbA1c and creatinine. On the other hand, alcohol consumption and job demand showed negative associations. It is also important to elucidate the significance of the above factors in the development of hypo-HDLcholesterolemia.
We are planning to further investigate the relationship between the above-noted factors and development of hypo-HDL-cholesterolemia in a longer prospective cohort study.
In this company, the workers who had abnormal finding at the annual health examination received the health guidance by a physician or an occupational health nurse. However, we consider such health guidance did not biased the results because of the adjustment for various factors related to the behavioral change by the health guidance, such as the body mass index, blood pressure, lifestyles and blood biochemistries.
In conclusion, using a pooled logistic regression analysis of the annual health examination data of about seven thousand Japanese male workers, this study demonstrated that elevated HsCRP is associated with the development of hypo-HDL-cholesterolemia.
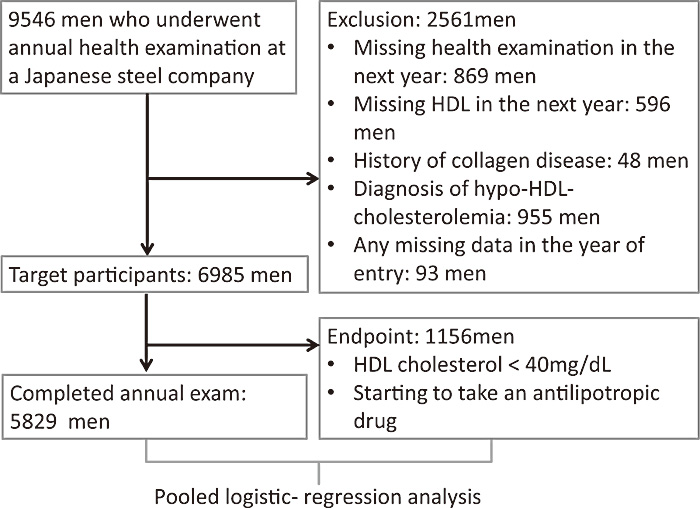
Fig. 1
Study design and participants
Abbreviations: aspartate aminotransferase (AST), body mass index (BMI), Brief Job Stress Questionnaire (BSJQ), confidence intervals (CI), geometric mean (GM), geometric standard deviation (GSD), high- sensitivity C-reactive protein (HsCRP), high-density-lipoprotein (HDL), odds ratios (OR), standard deviation (SD)
Address correspondence to Dr. Yasushi Suwazono.
Department of Occupational and Environmental Medicine,
Graduate School of Medicine, Chiba University, 1-8-1,
Inohana, Chuou-ku, Chiba, 260-8670 Japan.
Phone: +81-43-226-2065. Fax: +81-43-226-2066.
E-mail
: suwa@faculty.chiba-u.jp
