




Chiba Medical J. 90E:7~12,2014
doi:10.20776/S03035476-90E-2-P7
[Case Report]
Masaki Norimoto, Seiji Ohtori, Yawara Eguchi, Gen Inoue, Sumihisa Orita, Kazuyo Yamauchi, Yasuchika Aoki, Junichi Nakamura, Tetsuhiro Ishikawa, Masayuki Miyagi, Hiroto Kamoda, Miyako Suzuki, Gou Kubota, Yoshihiro Sakuma, Yasuhiro Oikawa, Kazuhide Inage, Takeshi Sainoh, Jun Sato, Tomoaki Toyone and Kazuhisa Takahashi
Department of Orthopedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
(Received December 27, 2013, Accepted January 31, 2014)
Intermittent parathyroid hormone (PTH) treatment reduces the risk for osteoporotic vertebral fractures. Preclinical data support the efficacy of PTH for lumbar spinal fusion. However, few clinical results investigating PTH for spinal fusion have been reported.
We report a 67-year-old female patient with osteoporosis, rheumatoid arthritis, and diabetic mellitus, who underwent posterolateral fusion using local bone grafting. Blood serum showed high levels of bone resorption marker. The patient underwent primary lumbar surgery and two additional lumbar surgeries during one year. Primary surgery was decompression and posterolateral fusion using local bone grafting with pedicle screws, and the subsequent second and third surgeries were performed due to proximal and distal adjacent problems. To address risk factors relating to bone union, daily subcutaneous injection of teriparatide was prescribed for one year. Low back and leg pain scores improved after final surgery. The final fusion level was from T9 to iliac. A large posterolateral fusion mass was observed in the lumbar area.
Daily subcutaneous injection of teriparatide using local bone grafting after instrumented lumbar posterolateral fusion was effective in a patient with risk factors for bone union.
Teriparatide, posterolateral fusion, lumbar, local bone, osteoporosis
Autologous iliac crest bone grafting is considered the standard criterion for lumbar spinal fusion. However, the outcome of autograft use in lumbar spine fusion is associated with donor site morbidity, such as risk of infection, hematoma, fracture, wound healing problems, and donor site pain. [1-5]To avoid donor site problems relating to lumbar fusion, local bone, ceramics, demineralized bone matrix, and bone morphogenetic proteins (BMPs) have been used. [6]
Three studies (two retrospective and one prospective) have reported that local bone graft and iliac crest bone graft showed no significant differences in fusion rate for one level fusion. [7-9] However, limitations of local bone grafts compared to iliac crest bone grafts for multiple level fusions have been reported. Retrospective and prospective studies have shown that fusion rates were poor for local bone graft alone in cases of more than three levels. [7,10]
Furthermore, many authors have reported risk factors that affect fusion in spine surgery including advanced age, sex, osteoporosis, smoking, diabetes mellitus, hypertension, revision surgery, multiple-level surgery, and medical comorbidities. [11,12]
Intermittent administration of parathyroid hormone (PTH) increases bone mass and reduces the risk of osteoporotic vertebral fractures. Recombinant human PTH (1-34) has already been approved as a treatment for severe osteoporosis. [13]Preclinical data in animal models support the use of PTH for lumbar spinal fusion. [14-16]Only one report has shown that daily subcutaneous injection of PTH (teriparatide) for bone union using local bone grafting after instrumented lumbar posterolateral fusion in postmenopausal women with osteoporosis was more effective than oral administration of bisphosphonate. [17]
In the current study, we report the clinical efficacy of teriparatide for bone union after instrumented lumbar posterolateral fusion using local bone grafting in a postmenopausal woman with risk factors for bone union such as osteoporosis, rheumatoid arthritis, and diabetic mellitus.
The protocols for human procedures used in this study were approved by the ethics committee of our institution. Written, signed consent was received from the patient before treatment.
In March 2011, a 69-year-old woman presented with a 3-year history of bilateral sciatica with complaints of pain in her buttocks and the lateral aspects of her legs. There was no apparent motor weakness. Sensory examination confirmed hypoalgesia in the lateral aspect of her upper and lower leg corresponding to the L4 and L5 dermatome. Bilateral straight leg raising test results were negative.
The patient had osteoporosis, rheumatoid arthritis, and diabetes mellitus. Young adult mean bone mineral density was 68% using dual energy x-ray absorptiometry (DEXA). The patient used 10mg of predonine for rheumatoid arthritis, and daily subcutaneous injection of insulin for diabetes mellitus. Laboratory data showed that white blood cell count was 7800/μl (normal range <8000) and C-reactive protein was 1.8mg/dl (normal range <0.3). Hemoglobin A1c was 7.2 (normal range <5.8%). The bone formation marker, bone alkaline phosphatase (BAP) was 6.0 (normal range: 7.9~ 29.0U/L) and the bone resorption marker, cross-linked N-telopeptide of type I collagen (NTX) was 35.0 (normal range: 7.5~16.5nmolBCE/L). In order to reduce the risk factors that may affect bone union, daily subcutaneous injection of teriparatide was performed from 3 months before first surgery to 9 months after first surgery.
X-ray examination showed L2 retro-spondylolisthesis, and L3 and L4 anterior spondylolisthesis (Fig. 1).
MRI could not be performed due to her brain clipping; however, mylogram and CT after myelography showed spinal stenosis form L2-3 to L4-5 (Fig. 2). As conservative treatment was not effective, surgery was planned. We performed decompression from L2-3 to L4-5 and posterolateral fusion with instrumentation at L2-L5.
Local bone consisting of lamina and spinal processes at the decompressed site was used and bone morphogenetic protein was not used during surgery (Fig. 3). The patient became symptom-free immediately after surgery, and the first 12 weeks post-operation were uneventful. However, the patient showed severe lower back and leg pain 12 weeks after surgery, and myelogram showed an adjacent segment problem and severe instability at L1-L2 level (Fig. 4). Therefore, in a second surgery we performed decompression at L1-2 with instrumentation at T9-L5.
Local bone consisting of lamina and spinal processes was used for posterolateral and interbody fusion at L1-L2 (Fig. 5). The patient became symptom-free immediately again after surgery. However, the patient showed severe lower back and leg pain 6 weeks after the second surgery, and myelogram showed an adjacent lower segment problem and severe stenosis at L5-S1 level (Fig. 6). Therefore, a third surgery was performed involving decompression at the L5-S1 level with addition of domino instrumentation to the iliac. Local bone from the L5-S1 level was used for posterolateral fusion at the L5-S1 level (Fig. 7). On a follow-up examination, the patient was symptom-free, and daily subcutaneous injection of teriparatide was performed for 1 year (3 months before first surgery to 9 months after first surgery), and a large posterolateral fusion mass was observed.
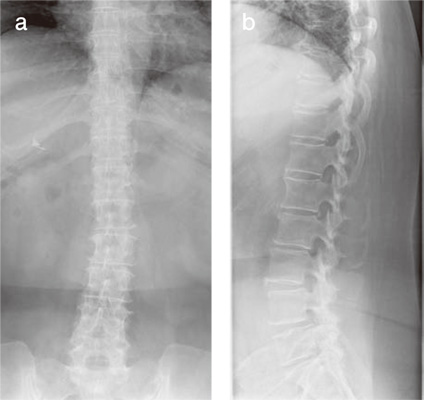
Fig.1
X-ray films showing thoracic and lumbar spine with osteoporosis. a: anterior-posterior view. b: profile view.
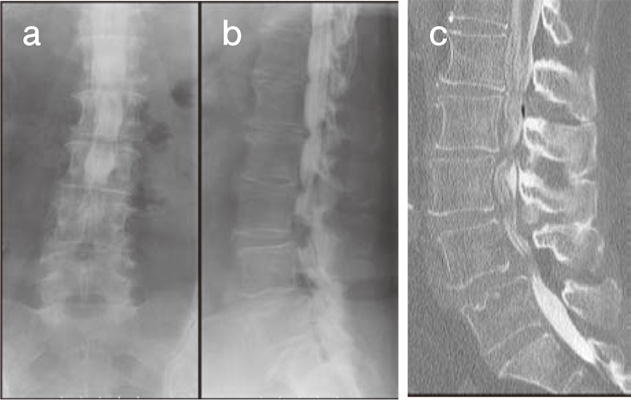
Fig.2
Mylogram and CT after myelography showed spinal stenosis form L2-3 to L4-5, and L2 retro- spondylolisthesis, and L3 and L4 anterior spondylolisthesis. a: anterior-posterior view. b: profile view. c: CT after myelography.
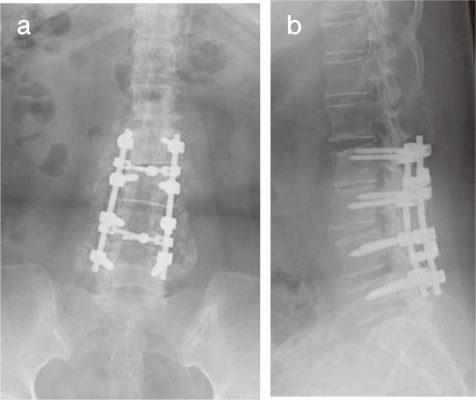
Fig.3
X-ray films after first surgery. Decompression from L2-3 to L4-5 and posterolateral fusion with instrumentation and local bone grafting was performed in the patient. a: anterior-posterior view. b: profile view.
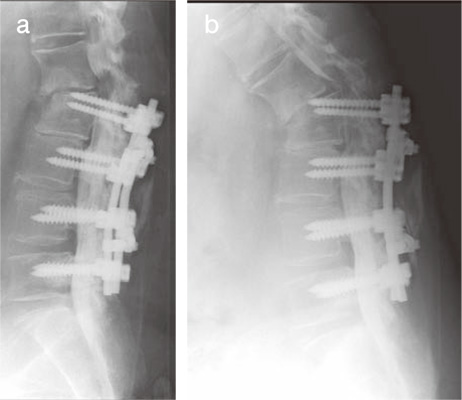
Fig.4
Myelogram showed upper adjacent segment problem and severe instability at L1-L2 level 3 months after first surgery. a: extended position. b: flexion position.
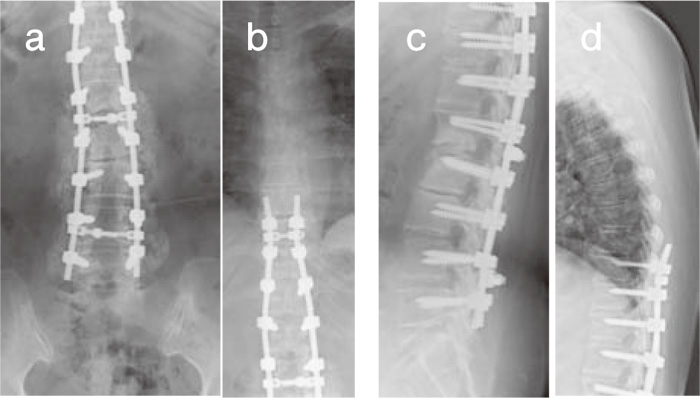
Fig.5
X-ray films after second surgery. Decompression at L1-2 with instrumentation and local bone grafting at T9-L5 was performed. a and b: anterior-posterior view. c and d: profile view.
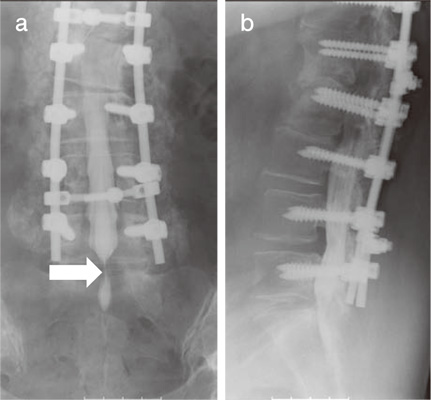
Fig.6
Myelogram showed lower adjacent segment problem (L5-S1) six weeks after second surgery. a: anteriorposterior view. b: profile view.
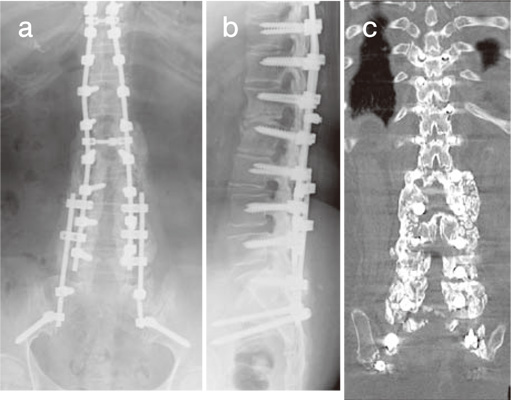
Fig.7
Figures show X-ray film and CT 9 months after third surgery. Decompression at L5-S1 level with addition of domino instrumentation to iliac was performed.
CT shows large bony mass at posterolateral region.
a: anterior-posterior view. b: profile view. c: coronal plane of CT.
In this case report, a 67-year-old woman with osteoporosis, rheumatoid arthritis, and diabetic mellitus underwent posterolateral fusion using local bone grafting accompanied by daily subcutaneous injection of teriparatide for one year. After one year, a large posterolateral fusion mass was observed.
Many authors have reported that risk factors that affect fusion in spine surgery include advanced age, sex, osteoporosis, smoking, diabetes mellitus, hypertension, revision surgery, multiple-level surgery, and medical comorbidities. [11,12]Therefore, we considered this patient at particularly high risk for poor bone union before surgery.
Preclinical data support the use of parathyroid hormone for lumbar spinal fusion. Teriparatide was shown to enhance spinal fusion using an autogenous iliac crest bone graft in a rabbit model of posterolateral fusion. [14,15]Intermittent administration of PTH enhanced bone turnover predominantly on bone formation at the graft site, accelerating spinal fusion using autologous bone grafts in rats that underwent posterolateral fuison. [16]To our knowledge, two clinical trial using teriparatide were reported in 2010 and 2011, respectively related to distal radial fractures and pelvic fractures. [18,19]Postmenopausal women, who had sustained a dorsally angulated distal radial fracture in need of closed reduction without surgery, were randomly assigned to eight weeks of once-daily injections of placebo or teriparatide. [18]The investigators concluded that healing time was shorter in the teriparatide-treated group. [18]In latter study, 65 elderly patients with osteoporosis had pelvic fractures. In this patient cohort, 21 patients received a once-daily injection of 100 μg PTH 1-84 starting within two days after admission to the hospital, and 44 patients served as the control group. PTH 1-84 was observed to accelerate fracture-healing in pelvic fractures and improved the functional outcome. Only one article has reported efficacy of teriparatide for fracture healing in cervical spine. [20]Three patients were observed to develop painful delayed unions of type III odontoid fractures despite external immobilization. All three teriparatide-treated patients experienced both rapid clinical improvement and computed tomography evidence of fracture union. [20]
The efficacy of daily subcutaneous injection of teriparatide for bone union using a local bone graft after instrumented lumbar posterolateral fusion in postmenopausal women with osteoporosis has been reported. [17]Teriparatide-treated patients showed superior results for the rate and average duration of bone union compared with bisphosphonate-treated patients.[17]However, the method of surgery was one-level or two-level posterolateral fusion. [17]In the current study, the patient had osteoporosis, rheumatoid arthritis, and diabetic mellitus, and underwent both primary lumbar surgery and two additional lumbar surgeries due to proximal and distal adjacent problems, and the final fusion level was from T9 to iliac. Bone resorption marker level was high in the patient. During surgery, we used only local bone. However, daily subcutaneous injection of teriparatide for 1 year enhanced large posterolateral fusion mass. Therefore, we concluded that combination of local bone and administration of teriparatide is useful for bone fusion in a patient with osteoporosis and some risk factors of non-union. The current study has limitations in that this is a single case report and the number of patients is restricted. Nevertheless, further studies are warranted into the efficacy of teriparatide to enhance spinal fusion in patients with osteoporosis.
There was no acknowledgment in the current study.
Address correspondence to Dr. Seiji Ohtori.
Department of Orthopedic Surgery, Graduate School of Medicine,
Chiba University, 1-8-1 Inohana, Chuo-ku, Chiba 260-8670, Japan.
Phone: +81-43-226-2117. Fax: +81-43-226-2116.
E-mail: sohtori@faculty.chiba-u.jp
