| 〔Case Report〕 |
Usefulness of Thumbtacks in Regulation for Massive Presacral
Hemorrhage in Rectal Surgery: Report of a case |
|
Masaki Nishimura, Keiji Koda, Kenji Oda, Kazuhiro Seike, Kimio Shimizu
Satoshi Fukutomi, Takehiko Sugihara, Hiroyuki Yoshidome and Masaru Miyazaki |
| (Received October 10, 2006, Accepted November 14, 2006) |
|
SUMMARY
We encountered a case who had massive presacral hemorrhage during rectal surgery. The patient was 86-year-old woman having carcinoma located at upper to middle rectum. Low anterior resection was planned to treat. When the tumor fixed to the pelvic lateral wall was mobilized by sharp dissection, massive bleeding occurred from presacral surface at S2 to S4 levels in the sacrum. Bleeding could not be easily controlled by conventional hemostatic maneuvers due to her narrow pelvis and heavy humpback. The only way to control bleeding was to press the fingertips on bleeding site, which temporarily controlled the bleeding. With sterilized metallic thumbtacks through an abdominal approach, bleeding was effectively controlled. There was no recurrence of bleeding and other complication in postoperative course. Thumbtacks is an useful tool to control massive presacral hemorrhage during rectal surgery.
|
|
Key Words
| Presacral hemorrhage, Thumbtacks, Rectal carcinoma |
|
| |
I. Introduction
During pelvic surgery, presacral hemorrhage is rarely seen. In case massive presacral hemorrhage occurs, it develops troublesome and occasionally life-threatening. Refractory presacral bleeding may be often difficult to be controlled with use of conventional hemostatic instruments including suture ligation, electrocautery, ligation and embolism of internal iliac vessels, and thrombogenic topical agents[1-4]. When these tools fail to control bleeding, pelvic packing with gauze is the only way to control massive bleeding through perineal approach, but the patient is likely to be susceptible to infection. Qinyao et al reported that hemostatic maneuver using sterilized metallic thumbtacks, for control for severe presacral hemorrhage[5]. Herein, we showed a case who had uncontrollable bleeding during rectal surgery but finally had successful hemostasis with thumbtacks.
II. Case
An 86-year- old woman was referred to our institution with complaint of constipation and anal bleeding. She had heavy humpback. Colonoscopy and radiological findings showed a rectal carcinoma located at upper to middle rectum. Proposed surgical procedure was low anterior resection. Laparotomy confirmed a large rectal tumor which was suspected to be adhered to presacral fascia, and narrow pelvic space due to her heavy humpback. Presacral bleeding was encountered when sharp dissection off the presacral fascia was performed for the tumor fixed to the right lateral and the posterior wall of the pelvis. Because of unexpected massive bleeding, we could not find the origin of massive bleeding in her pelvic space. Temporary gauze packing by the fingertip was performed at the bleeding site and tumor was resected as early as possible. After resection of the tumor, massive presacral bleeding seemed to be originated from presacral venous plexus at S2 to S4 levels. Bleeding was unable to be controlled despite conventional attempts including gauze packing, suture ligation, and cauterization except the finger pressure over gauze pad. We found out a chance using sterilized metallic thumbtacks, “Hemorrhage Occluder TM Pin” (Surgin, Inc. Tustin, CA) , to expect effective hemostasis. However, it was not available in our operating room, and we urgently placed an order. Hemostatic maneuvers were continued until its arrival. Presacral bleeding site was deep due to her narrow pelvis and heavy humpback, therefore, the procedure was changed to abdominoperineal approach in a lithotomy position. Unfortunately, massive bleeding was still uncontrollable despite with conventional hemostatic attempts through the perineal incision. Two hours after an order, thumbtacks was available and on the malleable applicator was immediately inserted into the sacrum at the sites of bleeding, obtaining controllable hemostasis (Fig. 1) . Other bleeding from presacral surface and braches of the right iliac vein was easy to be controlled by conventional hemostatic maneuver under direct visualization. Total blood loss was 9,365 ml, and intraoperative fluid replacement comprised 40 units of concentrated red blood cells, 18 units of fresh frozen plasma, and 10 units of platelets. There was no recurrence of bleeding and other complications. She had uneventful postoperative course without infection, and was discharged on 14 days after surgery.
|
 |
 |
Fig. 1
Radiograph of the pelvis showed thumbtacks inserted into the sacrum. |
Fig. 2
The schema of the sacrum. Each Arrows show the correspondence of basivertebral veins and foramen in each levels of the sacrum.
|
|
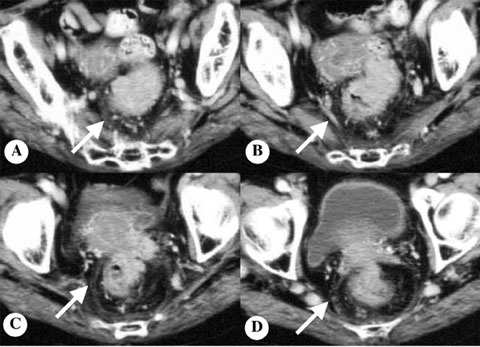 |
Fig. 3
Consecutive enhanced computed tomography of the rectal carcinoma. Fascia propria of the rectum (arrow in A-D) and vessel derived from the internal iliac vein (arrow in B) is drawn to the tumor. Fascia propria of the rectum has abundant blood flow due to tumor invasion.
|
|
III. Discussion
Recently, there is low morbidity and complication in rectal surgery because of recent advances in surgical techniques[5,6]. Presacral massive bleeding is still concerned as unfavorable complication. When presacral massive bleeding is encountered, suture ligation, electric cautery, ligation of the internal iliac vessels[1,2], selective arterial embolism[3], thrombogenic topical agents[4], inflatable balloon devices[7-9], pelvic packing, and use of thumbtacks[5,10,11]have been proposed for hemostatic maneuvers. In the present case, although conventional hemostatic tools including suture ligation and electro cautery were invalid for control of refractory presacral hemorrhage, gauze packing by the fingertip was temporarily effective for control of hemorrhage.
Qinyao et al reported that most of presacral hemorrhage occurr at presacral venous plexus which is covered by the presacral fascia. Basivertebral veins traverse the body of the sacrum through the sacral foramina overlying anterior surfaces of the third to fifth sacral vertebrae, which connect without venous valve [5](Fig. 2) . The most common cause of severe hemorrhage is laceration of basivertebral veins together with presacral venous plexus by the conventional procedure of blunt dissection in the retrorectal potential space by blindly stripping the posterior rectal wall from the sacral concavity[5,12,13]. Since the high hydrostatic pressure of the venous pool which is formed by basivertebral veins, presacral venous plexus, and the internal vertebral venous system can reach as high as approximately double or triple of the pressure of the inferior vena cava due to anesthesia and lithotomy position, refractory presacral hemorrhage may occur easily. In addition, Zama et al reported that expecting factors of massive blood loss were the fixation of the tumor, preoperative radiation, previous pelvic surgery, and more likely distal lesion of the rectum[13]. In the present case, the tumor developed clearly into mesorectum from findings of increasing vascularity and fat density in the mesorectum in preoperative enhanced computerized tomography (Fig. 3) . However, as the finding of the retraction of fascia propria to the tumor was seen in retrospective image evaluation, we may have to consider well that the tumor appeared to develop beyond mesorectum and fixed to presacral fascia. When surgeons consider possibility of refractory hemorrhage during mobilization of the rectum, it might be necessary to prepare for unordinary hemostasic maneuver including thumbtacks.
Currently, common useful hemostatic methods for refractory presacral bleeding are pelvic packing, thumbtacks, and muscle fragment (Table 1) . Although pelvic packing is the common conventional method for presacral bleeding, management after packing would be more complicated than other methods. Thumbtacks are useful in control of bleeding by which are placed directly over the bleeding point in the presacral fascia and pushed into the sacrum with the thumb. Compared with other methods, the advantage of thumbtacks is to achieve quick hemostasis. However, thumbtacks have disadvantages of the potential for displacement[14], not be overlapped when the hemorrhage is diffuse[15], not be readily available in most operating room, and application difficulty at the curved sacrum (levels S3 and S4) .
For massive presacral bleeding, Xu et al reported the latest hemostatic technique with a muscle fragment about 1.5 to 2.0cm in size, which is taken from the rectus abdominis[5]. The pressure with the fragment instead of the fingertip is controllable for bleeding and the indirect electro-coagulation through the fragment held in a long hemostatic forceps could stop bleeding. In a review of literature, this maneuver showed quick and permanent hemostasis with multiple bleeding sites without complications[16,17]. However, fragment which welds to bleeding site takes more than a minute[6,17]. For massive presacral bleeding from multiple sites such as the present case, hemostasis by the muscle fragment may be more difficult to be completed than by thumbtacks, technically.
In conclusion, there has not been a complete hemostatic attempt for every massive presacral hemorrhage in rectal mobilization. With full knowledge of pelvic anatomy in each case, pelvic surgeons should sufficiently evaluate local findings in preoperative images and get accustomed to several hemostatic tools for various presacral hemorrhages. When pelvic surgery with disadvantageous factors including narrow pelvis and humpback in addition to the fixation of the tumor to pelvic wall, it seems necessary to prepare for the thumbtack in advance..
|
|
|
要旨
症例は亀背の顕著な86歳女性。平成16年1月より腹痛,嘔吐出現。近医にて腸閉塞と診断され,入院後精査にてRasに半周性の2型腫瘍を認め,直腸癌の診断にて2月18日当科転院となった。術前精査で遠隔転移なし。3月15日手術施行。腫瘍は後腹膜と子宮へ癒着し可動性不良であった。TMEの層で直腸背側の剥離を進め,腫瘍の後腹膜への癒着部を剥離した際,仙骨前面静脈叢より大量の噴出性出血を生じた。腫瘍が大きく亀背のため骨盤内の視野が取れず,出血点の同定が困難であったため,まずガーゼパッキングを行った。占拠する腫瘍の切除をしないと出血点の同定は不可能と考え,後面は出血点近傍をガーゼで抑えながら可及的に剥離を進め,高位前方切除を施行した。出血部を検索したところ,S2からS4の怒張した仙骨前面静脈叢に複数の裂創を認めた。亀背と狭骨盤の症例であり,腹側から仙骨前面の視野が取りづらく止血操作は困難であった。仙骨ピンでの止血を試みるが院内に在庫なく,急遽製造元に手配を行った。その間術式をMiles手術に変更し会陰側から止血操作を試みたが止血には至らなかった。再び腹側へ移り仙骨ピンを合計7本使用し止血が可能となった。既に大量出血と大量輸血による出血傾向のため骨盤側面からの出血も認めたが,これらは腹側会陰側からの縫合結紮により止血可能であった。仙骨前面にタココンブ貼付し,会陰部開放創からガーゼパッキング施行後,人工肛門を造設し終刀した。術中出血量は9365gであった。術後人工呼吸管理を行い,第3病日に全身麻酔下にガーゼを除去した。骨盤内は完全に止血されており後出血も認めず,第14病日に退院となった。
|
|
References
1) Seavers R, Lynch J, Ballard R, Jernigan S, Johnson J. Hypogastirc artery ligation for uncontrollable hemorrhage in acute pelvic trauma. Surgery 1964; 55: 516-19.
2) Steinhart L, Hlava A, Navratil P, Svab J. Indications for obliteration of pelvic arteries in bleeding lesions of pelvic organs. In: Veiga-Pires JA, ed. Intervention radiology Amsterdam: Excerpta Medica 1980; 111-67.
3) Miller FJ Jr, Mortel R, Man WJ, Jahshan AE. Selective arterial embolization for control of hemorrhage in pelvic malignancy: femoral and branchial catheter approaches. AJR 1976; 126: 1028-32.[PubMed]
4) Losanoff JE, Richman BW, Jones JW. Cyanoacrylate adhesive in management of severe presacral bleeding. Dis Colon Rectum 2002; 45: 1118-9.[PubMed]
5) Qinyao W, Weijin S, Youren Z, Wenqing Z, Zhengrui H. New concepts in severe presacral hemorrhage during proctectomy. Arch Surg 1985; 120: 1013-20.[PubMed]
6) Xu J, Lin J. Control of presacral hemorrhage with electrocautery through a muscle fragment pressed on the bleeding vein. J Am Coll Surg 1994; 179: 351-2.[PubMed]
7)Cosman BC, Lackides GA, Fischer DP, Eskenazi LB. Use of tissue expander for tamponade of presacral hemorrhage: report of a case. Dis Colon Rectum 1994; 37: 723-6.[PubMed]
8) McCourtney JS, Hussain N, Mackenzie I. Balloon tamponade for control of massive presacral hemorrhage. Br J Surg 1996; 83: 222.
9) Braley SC, Schneider PD, Bold RJ, Goodnight JE Jr, Khatri VP. Controlled tamponade of severe presacral venous hemorrhage: use of a breast implant sizer. Dis Colon Rectum 2002; 45: 140-2.
10) Patsner B, Orr JW Jr. Intractable venous sacral hemorrhage: Use of stainless steel thumbtacks to obtain hemostasis. Am J Obstet Gynecol 1990; 162: 452.[PubMed]
11) Khan FA, Fang DT, Nivatvongs S. Management of presacral bleeding during rectal resection. Surg Gynecol Obstet 1987; 165: 274-6.
12) Nivatvongs S, Fang DT. The use of thumbtacks to stop massive presacral hemorrhage. Dis Colon Rectum 1986; 29: 589-90.[PubMed]
13) Zama N, Fazio V, Jagelman D, Lavery IC, Weakley FL, Church JM. Efficacy of pelvic packing in maintaining hemostasis after rectal excision for cancer. Dis Colon Rectum 1988; 31: 923-8.
14) Suh M, Shaikh J, Dixon AM, Smialek JE. Failure of thumbtacks used in control of presacral hemorrhage. Am J Forensic Med Pathol 1992; 13: 324-5.
15) Stolfi VM, Milsom JW, Lavery IC, Oakley JR, Church JM, Fazio VW. Newly designed occluder pin for presacral hemorrhage. Dis Colon Rectum 1992; 35: 166-9.[PubMed]
16) Harrison JL, Hooks VH, Pearl RK, Cheape JD, Lawrence MA, Orsay CP, Abcarian H. Muscle fragment welding for control of massive presacral bleeding during rectal mobilization: a review of eight cases. Dis Colon Rectum 2003; 46: 1115-7.
17) Ayuste E Jr, Roxas MF. Validating the use of rectus muscle fragment welding to control presacral bleeding during rectal mobilization. Asian J Surg 2004; 27: 18-21.[ELSEVIER]
|
|
Others
Department of General Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
西村真樹,幸田圭史,小田健司,清家和裕,清水公雄,福富 聡,杉原毅彦,吉留博之,宮崎 勝: 仙骨ピンでコントロールし得た仙骨前面多量出血の1例.
千葉大学大学院医学研究院臓器制御外科学
Tel. 043-226-2103. Fax. 043-226-2552. E-mail: m-nishimura@umin.ac.jp
2006年10月10日受付,2006年11月14日受理.
|
|
|
|
|
|
|
|
|
|