




Volume 84, Number 1
doi:10.20776/S03035476-84-1-P15
[Original Paper]
Harufumi Makino1), Shin-ichi Okazumi2), Shin-ichi Miyazaki2)
Hideki Hayashi1), Hideaki Miyauchi2), Satoshi Chiba5)
Ryoyu Mochizuki2), Takanori Shimizu2), Masato Endo3)
Yoshifumi Matsui4), Yuji Sugamoto6)
Takenori Ochiai2) and Tatsuo Igarashi1)
(Received July 9, 2007, Accepted July 24, 2007)
The port wound metastasis and distant metastasis may partly be caused by perioperative cancer-cell seeding. We report our technique for laparoscopic rectosigmoid colon resection using a medial approach as no-touch surgery. Twenty-three patients were carried out no-touch anterior resections using a laparoscopic medial approach. To prevent such spillage during colorectal surgery, we performed primary vascular pedicle ligation and occlusion of the distal colon and the mesocolon with Tetron-lined tape to provide dissection of the colon without tumor manipulation. Excellent postoperative outcome were observed in all patients. We believed that no-touch laparoscopic anterior resection for colorectal cancer can be performed safely and has beneficial effect on cancer recurrence. Long-term follow-up will be necessary to determine the effectiveness of this procedure for colorectal cancer.
Colorectal cancer, Laparoscopic surgery, No-touch isolation technique
Distant matastases after colorectal resection may be explained by spread of cancer cells from main tumor to regional lymph nodes and to liver or other organ. Lateral approach for rectosigmoid cancer mobilized main tumor at the start. It may cause perioperative hematogenous cancer cell seeding. To prevent such spillage during colorectal surgery, no-touch isolation technique with primary vascular ligation has been developed. We found that the medial approach to laparoscopic anterior resection provides the primary ligation of vessels without mobilization of main tumor. In this study, we report our technique for laparoscopic rectosigmoid colon resection using a medial approach as no-touch surgery.
Between July 2002 and December 2003, twenty-three patients were carried out anterior resections using a laparoscopic medial approach. The patients consisted 16 males and 7 females with ages ranging between 50 and 80 (average 64.0 years). The procedures were performed for twenty sigmoid colon cancers and three rectal cancers. The same surgeon (HM) performed all procedures.
Under general anesthesia, the patient was placed supine in the lithotomy position. The operation was begun in the Trendelenburg position (20-degree head down tilt), and the patient was tilted to the right side so that the small bowel fell down the right upper quadrant of the abdominal cavity, creating an unobstructed operating field. Video monitor was placed at the foot of the table to the left of the patient. The surgeon and the camera operator stood on the patient’s right side, with first assistant on the patient’s left side. At first, 12-mm trocar had been placed supraumbilically and another two trocars (a right upper abdominal, right lower abdominal [12mm each] ) were placed. If forth trocar is needed for an extra instrument, it is placed in the left lower abdomen. A 10-mm, 30-degree-angle laparoscope was induced through the right upper abdominal trocar.
The retroperitoneum is incised just above the aortic bifurcation and the incision is extended toward the origin of the inferior mesenteric artery. And the inferior mesenteric artery and vein are divided primarily to prevent spreading of cancer cells to the portal vein. The origin of the inferior mesenteric artery is divided using double clips and ultrasonic dissector. The inferior mesenteric vein and the left colonic artery divided same procedure at same level of the origin of the inferior mesenteric artery (Fig. 1). Because of the dissection of the sigmoid mesocolon is performed above prerenal fascia, the right ureter and right gonadal vessels covered with retroperitoneal fat are visualized clearly under the prerenal fascia. Also lumber splanchnic nerves and hypo gastric nerves are preserved as logical consequence. Most of the planes of dissection are avascular, and the dissection can be performed safely using an electrocautery attached dissector or an ultrasonic dissector. The peritoneum of the left side of the sigmoid and descending colon is incised to mobilize tumorous lesion completely.
In the next step, the distal colon and the mesocolon of the tumor is ligated with Tetron-lined tape to occlude. The distal colon can be retracted any direction with the tape. This makes dissection of mesorectum extremely easy and need not any touch to the tumorous lesion (Fig. 2). The mesorectum is dissected, starting with posterior mobilization, followed by dissection posterolaterally to the right and left of the rectum. This approach carried out by ultrasonic dissector down to the distal resection line. After the rectum is freed from pelvic wall, the mesorectum is divided using ultrasonic dissector without clips. The distal rectum wash out is performed transanally. And the distal rectum is transected with a reticulated endoscopic stapler. The supraumbilically trocar site is widened by 5 cm, and plastic wound protector is attached on abdominal wall to prevent exposing any abdominal tissue to tumorous lesion. The proximal rectum is delivered through this incision, and the specimen is resected. The anvil of the EEA stapler is inserted into the lumen of the colon and secured in place with a purse-string stitch. This end of colon is returned to abdomen, closing the extended incision. The anastomosis is created by standard double-stapling technique (Fig. 3). A drain is placed through the right lower trocar site and the operation is completed.

Fig. 1
The origin of the inferior mesenteric artery is divided using double clips and ultrasonic dissector. The inferior mesenteric vein is divided same procedure at same lever of the origin of the inferior mesenteric artery.
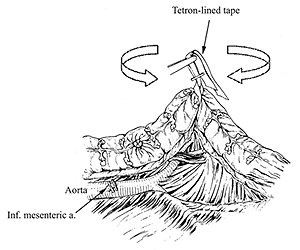
Fig. 2
The distal colon and the mesocolon are ligated with Tetron-lined tape to occlude. The distal colon can be retracted any direction with the tape.
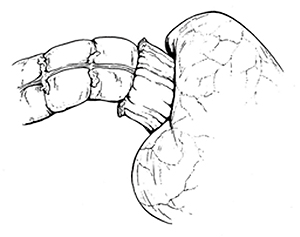
Fig. 3
The anastomosis is created by standard double-stapling technique.
Median operative time was 204 minutes (range 110 to 310). Of the twenty-three patients, eight had the procedure using only three trocars, and fourteen patients required placement of four trocars, only one patient needed five trocars. None of the patients required an open procedure.
Mean hospital stay was 9.0 days (range 7 to 14). Mean blood loss was 61.5 ml (range 0 to 350). Mean number of harvested lymph nodes per patient was 18.9 (range 5 to 48) (by pathologist).
Pathologic examination of the specimen revealed according to Union Internationale Contre le Cancer TMN classification, six patients were pT1, pN0, pM0, stage I; five patients were pT3, pN0, pM0, stage II; and one patient was pT1 pN1, pM0, one patient was pT2, pN1, pM0, two patients were pT3, pN1, pM0, three patients were pT3, pN2, pM0, three patients were pT4, pN1, pM0, two patients were pT4, pN2, pM0, stage III. Although the average follow-up period was 11.3 months (range 4 to 21 months), no patients had developed recurrence of disease according to ultrasonography, CT, and colonoscopy.
Excellent postoperative outcome were observed in all patients. There was no mortality during the perioperative periods. All patient reserved normal urinary function and pre operative level of sexual function, according to the questionnaire.
Since the introduction of laparoscopic colon surgery in 1991, many surgeons have adopted laparoscopic colon surgery to reduce invasiveness [1]. However, numerous reports of the development of port wound metastasis were described [2]. Early reports were reviewed that laparoscopic surgical procedures may increase the risk of the port wound metastasis. In recent years several authors reported that tumor manipulation increased tumor metastasis. On the other hand, distant metastasis after colorectal surgery may be explained by spread of cancer cells to regional lymph nodes and to the liver via lymphatics and the portal vein [3-7]. The port wound metastasis and distant metastasis may partly be caused by perioperative cancer-cell seeding. Furthermore it is obvious, intraoperative manipulation of tumorous lesion promotes spread of cancer cells. To prevent such spillage during colorectal surgery, no-touch isolation technique with primary vascular ligation has been developed. In our technique, we performed primary vascular pedicle ligation and occlusion of the distal colon and the mesocolon with Tetron-lined tape to provide dissection of the colon without tumor manipulation. It is widely accepted that laparoscopic surgical procedure has many advantages that less pain, early mobilization, better cosmesis, and shorter hospitalization over open surgery.
We believed that no-touch laparoscopic anterior resection for colorectal cancer can be performed safely and have beneficial effect on cancer recurrence.
Long-term follow-up will be necessary to determine the effectiveness of this procedure for colorectal cancer.
【目的】大腸癌治療においてNo-touch Isolation Techniqueの概念に基づき, No-touch Laparoscopic Anterior Resectionを行い, その有用性を検討する。
【対象】2002年7月より2003年12月までに, 腹腔鏡下前方切除術を内側アプローチおよびNo-Touch Isolation Techniqueを用いて手術を行った, S状結腸癌および上部直腸癌, 男性16例, 女性7例の23例。年齢: 50~80歳 (平均年齢64.0歳)
【方法】腹腔鏡下にて内側アプローチを用いS状結腸および直腸を受動した後, 術中の腫瘍細胞の播種を予防するため, 腫瘍の流入流出血管の結紮・切離と腫瘍の肛門側の腸管の遮断を行った。
【結果】平均手術時間204分 (110~310分) 。術中偶発症および開腹移行例0例。平均術後在院日数9.0日 (7~14日) 。平均出血量61.5, ml (0~350ml) 。平均郭清リンパ節数18.9個 (5~48個) 。と良好な結果を得た。
【考察】大腸癌治療におけるNo-touch Laparoscopic Anterior Resectionの安全性と有用性が示唆された。また, No-touch Laparoscopic Anterior Resectionは術中の腫瘍細胞の播種を防ぐ可能性があり, 今後長期の経過観察が必要と考えられた。
1) Section for Medical Robotics and Surgical Device Creation, Research Center for Frontier Medical Engineering, Chiba University, Chiba 263-8522.
2) Department of Frontier Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
3) Department of Surgery, JA Saitama Koseiren Kumagaya General Hospital, Saitama 360-8567.
4) Department of Surgery, JA Shizuoka Koseiren Shimizu Kosei Hospital, Shizuoka 424-0193.
5) Department of Surgery, Naruto General Hospital, Chiba 289-1326.
6) Department of Surgery, Numadu City Hospital, Shizuoka 410-0302.
牧野治文1), 岡住慎一2), 宮崎信一2), 林 秀樹1), 宮内英聡2), 千葉 聡5), 望月亮祐2),
清水孝徳2), 遠藤正人3), 松井芳文4), 菅本祐司6), 落合武徳2), 五十嵐辰男1):
大腸癌に対するNo-touch Laparoscopic Anterior Resection.
1) 千葉大学フロンティアメディカル工学研究開発センター手術・生体機能支援機器研究部門
2) 千葉大学大学院医学研究院先端応用外科学, 3) 熊谷総合病院外科,
4) 清水厚生病院外科, 5) 成東病院外科, 6) 沼津市立病院外科
Tel & Fax. 043-290-3117. E-mail: fwhp4815@mb.infoweb.ne.jp
2007年7月9日受付, 2007年7月24日受理.
