




Volume 85, Number 3
doi:10.20776/S03035476-85-3-P125
[Original Paper]
Yukiko Neff1), Hideaki Bujo2), Yo Miyashita3), Daigaku Uchida4)
Toshiaki Ban5), Jun Tashiro6,7), Kenya Yamazaki7), Ko Ishikawa8)
Takahiko Tokuyama8), Meizi Jiang2), Toru Kawamura1) and Yasushi Saito1)
(Received December 11, 2008, Accepted January 23, 2009)
The aim of this study was to investigate the significance of patient awareness regarding one’s own medical data, relative to the improvement of their life style-related diseases. The awareness scores of 702 patients were represented by counting the number of “yes” to the question “Do you know your values for following issue?” for the value of physical data, biochemical data, or instructed intake calorie, and they were analyzed in relation to the evaluation scores determined by their physicians after six months. The evaluation score in the group of subjects aware of the issues of body weight, waist circumference, blood pressure, total cholesterol, HDL-cholesterol, triglyceride, glucose, HbA1c, and caloric intake were significantly increased in comparison to those in the group without the awareness. The evaluation scores in subjects with an awareness score of more than 3 in males and more than 5 in females were significantly higher than those of subjects with an awareness of 2 and 1, respectively. A multivariate analysis showed that waist circumference and blood pressure in all, HbA1c and HDL-C in the biochemical, and caloric intake and blood pressure in the physical and instruction issues were significantly associated with the evaluation scores. Thus, an increase in patients’ awareness may contribute to improvements in the management of lifestyle-related diseases.
awareness, patient, lifestyle-related disease, improvement, management
The concept of a metabolic syndrome has been established in many countries as a risk for the development of cardiovascular diseases or diabetes mellitus[1-4]. The subjects with metabolic syndrome are generally at first encouraged to manage their lifestyle correctly in order to keep their body weight, blood pressure, plasma lipids, and plasma glucose within normal ranges, according to the guidelines in health-promoting programs[1-4].
Previous studies have shown that lifestyle intervention is effective for the prevention of cardiovascular diseases or diabetes mellitus, even though the pathogenesis is believed to result from the accumulation of inherited factors which determine the probability of developing the lifestyle related diseases[5-9]. One of the most evident interventions is long-term weight reduction through a combination of dietary modification and exercise[10-12]. The outcomes of these lifestyle modification studies are sometimes equal to, or more effective than, those using anti-hypertensive, anti-dyslipidemic, or anti-diabetic drugs for the patients with a high risk for cardiovascular diseases[5,6]. However, an issue which remains to be resolved is how the desired outcome can be successfully obtained in the medical practice setting between patients and physicians, involving the prevention of drop-out subjects in health-promoting projects, the achievement of recommended diet and/or exercise programs, and the assessment of data as self-reported by patients.
One of the major factors negatively affecting the achievement of outcomes expected for patients with lifestyle-related diseases is the heterogeneity in their awareness (or recognition) of their current disease conditions and/or risks for cardiovascular diseases or diabetes mellitus[13-16]. The inadequate awareness of their own conditions, even by those patients who continue regular hospital visits for health maintenance and pharmacological intervention when needed, may reduce the efficiency of disease management based on the relationship between patients and physicians. In this context, there is only limited information about the significance of awareness and/or patients’ personal understanding of values related to physical and biochemical data, as well as physician-recommended dietary programs. Population studies have suggested that patients’ awareness of their own values is related to the adequate control of lifestyle-related diseases, such as hypertension, dyslipidemia, and diabetes mellitus[13,15,16]. Thus, to be aware of one’s own medical data may be a key factor in improving the efficiency and management of lifestyle-related diseases during the regular hospital visits.
The current study aimed to investigate the significance of the awareness of patients of their abnormal physical findings, biochemical values, and recommended intake of calories for the improvement of hypertension, dyslipidemia, or diabetes mellitus. The data from patients in seven hospitals were obtained from a questionnaire focusing on the patients’ awareness of their physical findings, biochemical examination, and intake of calories, and were analyzed in relation to the evaluation scores as determined by their physicians after six months based on data obtained from seven hospitals.
The study was carried out from September 2006 to August 2007 in seven hospitals in Chiba prefecture and included 1023 patients between 40 and 80 years of age who were diagnosed as having lifestyle-related diseases, consisting of hypertension, dyslipidemia, and diabetes mellitus. The diagnoses of these diseases were determined according to the guidelines for hypertension, dyslipidemia, or diabetes mellitus in Japan[17-19]. The questionnaires were handed out to these patients on their first visit, and were collected on the same day with a mark response on “Yes” or “No” to each issue question (Fig. 1). Participants were considered to be aware of the issue if they answered “yes” to the question “Do you know your values for following issue?” The questioned issues were the values of body weight, waist circumference, blood pressure, total cholesterol (TC), HDL-cholesterol (HDL-C), triglyceride (TG), glucose, HbA1c, and the caloric intake recommended by their physicians. The answers with no or both mark(s) on “Yes” and “No”, and the answers with a mark(s) at inappropriate spaces were categorized as “Others”. The sum of question issues with “Yes” among the 9 issues was defined as “Awareness score” with the range of 0 at minimum to 9 at maximum. Each physician continued to monitor their patients during the next six months without changing the contents or amount of prescribing drugs nor the instruction of life-style modification by physicians and other medical instructors, and provided an evaluation for the patients’ health condition using a score from 1 (worst) to 5 (best). Any patients who stopped visiting the hospitals or whose medication was changed during the 6-month period were excluded from the study. The “Evaluation score” was based on any change during the 6-month period in one of the above issue values (except caloric intake) the most tightly concerning the treatment of patients: levels 1, 2, 3, 4, and 5 indicates the changes of values more than 15 % worse, 15 % to 5 % worse, 5 % worse to 5 % better, 5 % to 15 % better, and more than 15 % better, respectively, than values measured in one month before the study (standards for evaluation after 6 months treatment). Eight physicians took part in this study, and the study design including evaluation methods were informed to all physicians at the meeting before the study. The physicians finally confirmed all patients have completed this study according to the above design after the six-month follow-up period.
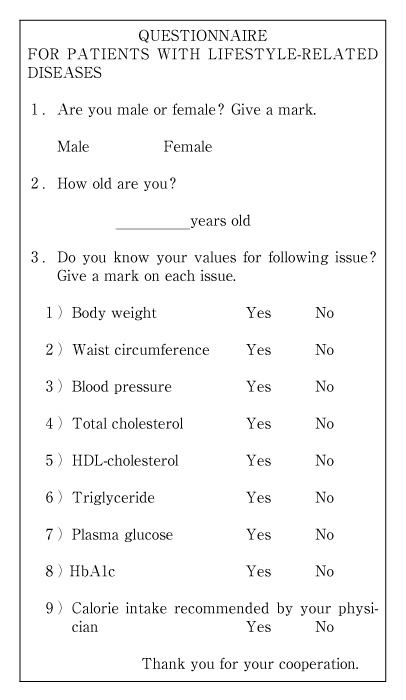
Fig. 1
The questionnaire used in this study. Note that the sentences were originally written in Japanese.
The statistical analysis was performed with the SPSS version 13.0 software program (SPSS Japan, Inc). The associations of the evaluation score with the awareness issues were examined by unpaired t-test. Multiple linear regression analyses were performed by controlling for age (10y increase), sex, and all issues (Model 1), biochemical issues (Model 2), or physical and instruction issues (Model 3). In the figures, the results are shown as the mean ± SD. A 1-way ANOVA was used to compare between two groups, and the Duncan multiple range test was used for the comparison of multiple groups. A value of P<0.05 was considered to be significant.
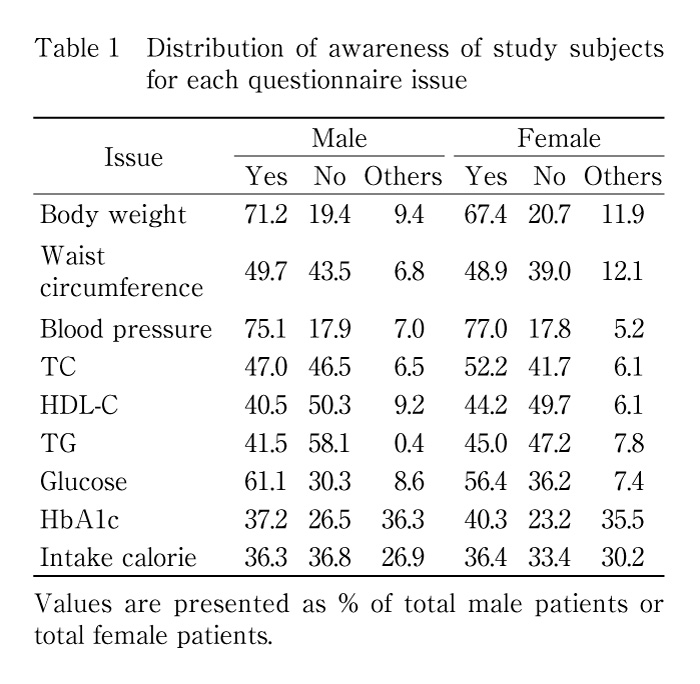
The questionnaires were given to 1023 patients with hypertension, dyslipidemia, or diabetes mellitus in 7 hospitals. 67 patients quitted the regular visiting to the hospital, and 231 patients changed the prescribed drugs in the following 6 months. As a result, the 725 patients were analyzed by physician’ evaluation scores. Of the initial 725 questionnaires, 702 were further analyzed, and 23 questionnaires were not analyzed due to insufficient data. The averaged age of analyzed patients was 61.2 ± 13.1 yr, the ratio of male to female subjects was approximately 1 : 1, and the range of ages was distributed from 40 to 80 years in both males and females. The proportions of patients with hypertension, dyslipidemia and diabetes were 71 %, 70 % and 53 %, respectively. The frequencies of “Yes” responses for the awareness of values in all subjects were 69.3 %, 49.3 %, 76.1 %, 48.5 %, 42.3 %, 43.3 %, 58.8 %, 38.8 %, and 36.4 % for body weight, waist circumference, blood pressure, TC, TG, HDL-C, glucose, HbA1c, and intake of calories, respectively (Table 1).
The frequency of “Yes” for the awareness of blood pressure was significantly higher in the subjects with hypertension than that in the subjects with dyslipidemia or diabetes (Table 2).
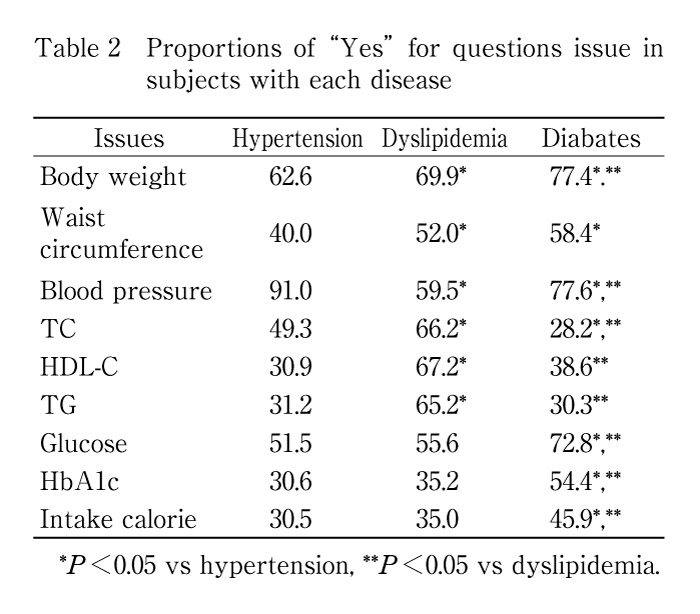
The frequencies of “Yes” for the awareness of TC, HDL-C and TG were significantly higher in the subjects with dyslipidemia than those in the subjects with hypertension or diabetes, respectively. The frequencies of “Yes” for the awareness of body weight, weight circumference, glucose, HbA1c and intake calorie were significantly higher in the subjects with diabetes than those in the subjects with hypertension or dyslipidemia, respectively. The averaged awareness scores were 4.3 ± 3.1 for the 702 patients, significantly higher than those for the above patients who dropped out of the study (3.1 ± 1.9, P<0.05). The frequencies of the evaluation scores from 1 (worst) to 5 (best) as evaluated by the physicians responsible for the patients were 3.5 % for 1, 14.2 % for 2, 38.3 % for 3, 29.5 % for 4, and 13.5 % for 5 in all subjects: No significant difference was observed among physicians regarding the frequencies of each evaluation score. The averaged evaluation scores were 3.4 ± 1.0 in males and 3.3 ± 1.0 in females (no significant difference between males and females).
In order to investigate the effect of patient awareness on the improvement of diseases treated in the hospital, we analyzed the relationship between the patients’ awareness scores and the physicians’ evaluation scores (Fig. 2). The evaluation scores tended to increase in conjunction with the awareness scores in both male and female subjects. The evaluation scores in subjects with an awareness score of more than 3 in males and more than 5 in females were significantly higher than those of subjects with an awareness of 2 and 1. These results suggest that the awareness scores are related to the evaluation scores for the 6-month follow-up care in hospitals.
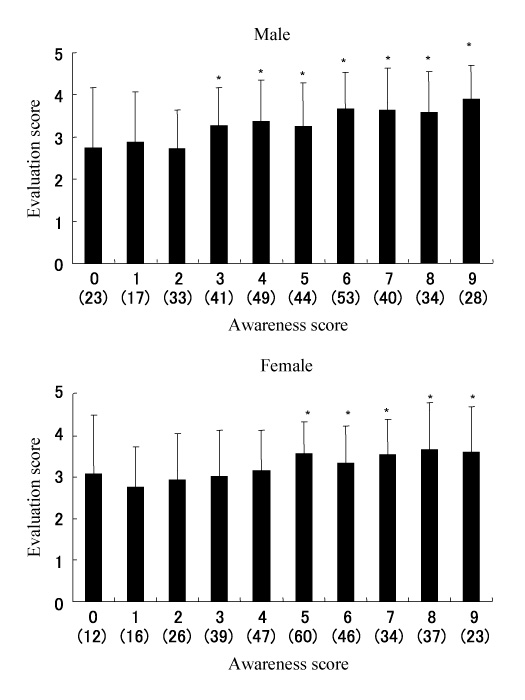
Fig. 2
Relationships between the sum of the awareness score and the evaluation score in males and females. Each score (Yes=1, No=0) of the issue was summed. Bars indicate the mean ± S.D. *P<0.05 vs awareness score 2 and 1 in males and females, respectively. The categorized subject numbers are shown in parenthesis.
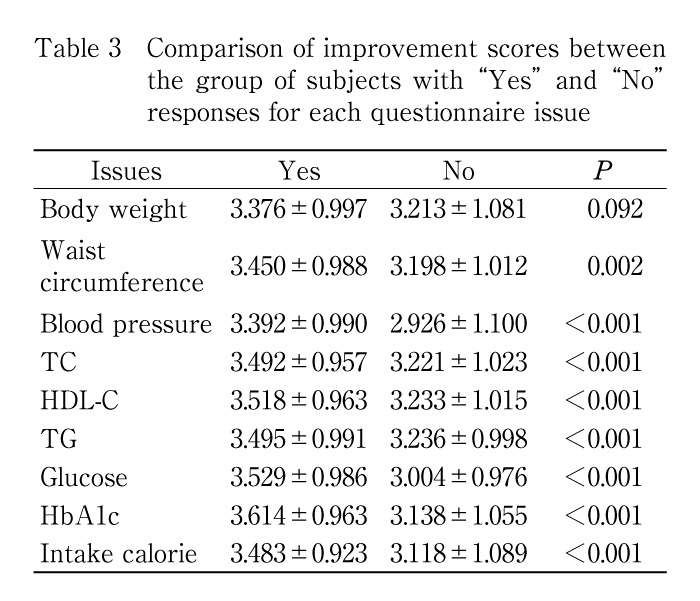
In order to investigate the relationship between the awareness of patients for each issue and the evaluation scores determined by physicians, we compared the evaluation scores between two groups of subjects with “Yes” or “No” for each of the following issues: body weight, waist circumference, blood pressure, TC, TG, HDL-C, glucose, HbA1c, and intake of calories (Table 3). The patients who answered “Yes” for awareness had significantly higher evaluation scores than those who answered “No” for awareness in all issues. The scores for patients who responded “Yes” for awareness of glucose, blood pressure, HbA1c, intake of calories, and HDL-C values were increased by 1.17, 1.16, 1.15, 1.12, and 1.09 fold, respectively, in comparison to those who answered “No.” These results suggest that patients who are aware of their own values, particularly, those of glucose, HbA1c, calorie intake, or HDL-C could thus have better disease management after 6 months.
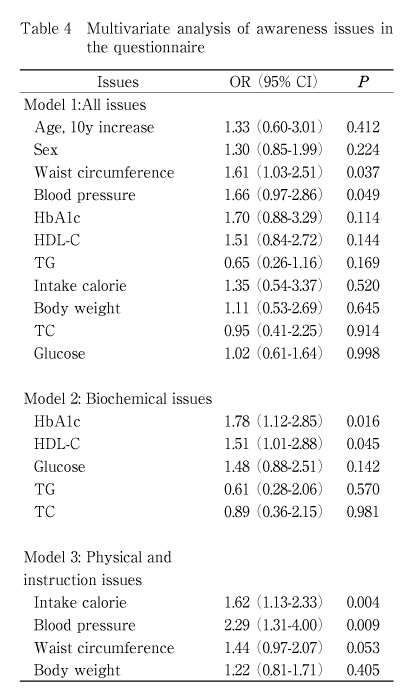
We next analyzed the multivariate independence of the issues for the improvement of diseases (Table 4). The awareness of waist circumference or blood pressure was significantly associated with the improvement of diseases after controlling age, sex, and all other issues. Next, the questionnaire data were analyzed after grouping variables according to biochemical, physical, and instruction issues. These analyses showed that HbA1c or HDL-C in the biochemical area, and caloric intake or blood pressure in the physical and instruction area were significantly associated with the evaluation scores after controlling for all other issues in each area, respectively. These results suggest that among all of these issues, certain ones are critical for the improvement of lifestyle-related diseases.
We finally analyzed the significance of the awareness of issues representative for each lifestyle-related disease for the improvement of the disease in these patients. For this purpose, the blood pressure, HDL-C, and glucose were chosen as the most frequently aware issues in all for the patients with hypertension, dyslipidemia, and diabetes mellitus, respectively, based on the results in Table 2. The relationship between the combination of these three representative issues and the evaluation scores was analyzed (Fig. 3). The evaluation scores tended to increase in conjunction with the increase in the sums of the representative awareness issues, as observed in the results in Fig. 2. Moreover, a statistically significant increase in the evaluation scores was observed in relation to the awareness for blood pressure or glucose; the evaluation scores of subjects with “Yes” for awareness only for blood pressure or glucose were significantly higher than those of subjects with “No” for awareness of all issues. On the other hand, the evaluation scores of subjects with “Yes” for awareness, only for HDL-C, were not increased in comparison to those of subjects with “No” for awareness of all issues. These results indicate that the awareness of specific issues, in addition to total disease awareness, is therefore an important contributing factor for the improvement of diseases.
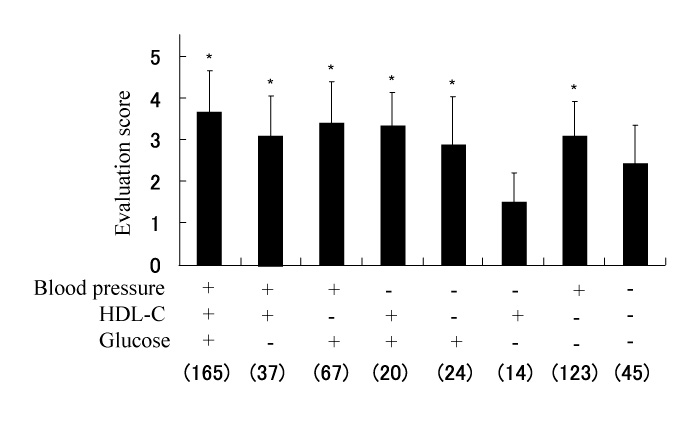
Fig. 3
Relationships between three representative common issues for hypertension, dyslipidemia, or diabetes mellitus in combination, and the evaluation score. Bars indicate the mean ± S.D. *P<0.05 vs “No” for blood pressure, HDL-C, and plasma glucose. The categorized subject numbers are shown in parenthesis.
Lifestyle modification has been shown to prevent atherosclerosis or diabetes mellitus for the patients with coronary artery diseases or glucose intolerance[5,6]. A recent follow-up study of patients with coronary diseases showed that the sustained intensive lifestyle changes led to greater regression of coronary atherosclerosis after five years than after only one year[6]. The regression in atherosclerosis after one year was accompanied with by a 37 % reduction in the plasma LDL-cholesterol (LDL-C) level in those subjects[6]. In contrast, coronary atherosclerosis continued to progress in the subjects without lifestyle changes[6]. These observations indicated that the achievement of lifestyle modification is important for the management of risk factors for atherosclerosis. Many factors which influence the achievement of lifestyle modification exist in the daily medical management between patients and physicians. One such factor may be patient awareness of the current condition of their disease. The awareness of patients for their current condition seems to, in part, depend on their recognition ability and appropriate environment, including the physicians’ instructions and treatment. The patients’ literacy or reading ability has been shown to be an important factor for predicting who will benefit from an intervention for diabetes management[20-22]. Population-based studies have suggested that the reduced awareness of people of their own values of plasma cholesterol or blood pressure is linked to an increase in the frequency of hypertension or hypercholesterolemia[13,14,16]. Another study showed that the knowledge of the risk factors for cardiovascular disease is important for effecting changes in the behavior of older people in their daily lives[15]. Consequently, the awareness in patients for the significance of abnormality in blood pressure, lipids, and glucose is expected to effect on the improvement of treatments for hypertension, dyslipidemia, and diabetes mellitus, respectively. The average age and the ratio of males and females of the subjects indicated that they were a representative group of patients regularly visiting hospitals for the treatment of hypertension, dyslipidemia, or diabetes mellitus, with or without cardiovascular diseases, in Japan. The analysis of the collected questionnaire data suggested that the evaluation score given by the physicians tended to increase in both males and females in parallel with the sum of all the awareness scores by the patients. The evaluation scores of these subjects with “Yes” responses were significantly higher than for those subjects who responded “No” for awareness in every issue. The logistic analysis of issues revealed that there were certain key factors for the evaluation scores: the waist circumference and blood pressure in all, HbA1c and HDL-C in biochemical, and intake calorie and blood pressure in physical and instructions. In particular, the awareness of blood pressure and glucose was effective for the disease improvement in comparison to that for HDL-C. These results indicate that a higher awareness of one’s own conditions can lead to the improvement of lifestyle-related diseases, as estimated by physicians. A representative marker, such as blood pressure, may serve as a key factor for the achievement of self-motivated lifestyle behavior modification, in addition to the increase in the sum of the awareness issues. This observation may be derived from the knowledge of patients that blood pressure serves as a marker of health disturbance, through years of medical education, and the common behavior of patients in monitoring their blood pressure at home. In addition to blood pressure, the knowledge of glucose level may indicate the depth of awareness of patients for the management of lifestyle-related diseases in comparison to HDL-C. The clinical significance of each issue in the questionnaire should be further analyzed in future studies involving a larger population and more detailed information about their disease conditions. One limitation of this study regarding the data interpretation is first that the physicians were not blinded for awareness scores when they provided evaluation scores for their patients. Therefore, the possibility of influence and bias for the evaluation scores by the facts that physicians were aware of their patients’ awareness is not able to exclude from the interpretation of study results. The second point to be considered is that the awareness scores at the first visit may changed in the followed 6 months before making evaluation scores. The improvement of patients’ awareness in the treatment period should be considered as an influencing factor for the improvement of their diseases. Third, the lack of data on the patients’ educational level and current or previous occupation is another limitation for the data analysis in our study, since the previous studies have shown close relationships to exist between literacy or reading ability and management of lifestyle-related diseases[20-22]. Finally, the control group without questionnaires of patients’ awareness was not included in the study design. The response of patients for the questionnaires itself may have influenced the study results, considered by the observation that the averaged awareness scores in the 702 completed patients were significantly higher than those for the patients who dropped out from the study (see Results). This study has shown that one of the major factors negatively affecting the achievement of outcomes expected for patients with lifestyle-related diseases is their reduced awareness (or recognition) level of their current disease conditions. Therefore, the physicians are suggested to consider that the patients’ awareness of their own conditions may reduce the efficiency of disease in the management of hypertension, dyslipidemia, and diabetes mellitus. It may improve the management conditions of lifestyle-related diseases to keep one’s own medical data on biochemical, physical, and instruction issues in patients’ mind during the regular hospital visits. In conclusion, the current study showed the significance of patients’ awareness for their conditions in the improvement of three lifestyle-related diseases, hypertension, dyslipidemia, or diabetes mellitus. It is therefore important for physicians to improve their efforts to help increase of the patients’ awareness and/or recognition of their current conditions since this would be effective for improving the treatment of patients in daily practice for lifestyle-related diseases.
This work was partly supported by Health and Labor Sciences Research Grants to H.B. and Y.S. for The Research of Primary Hyperlipidemia from the Ministry of Health, Labour and Welfare, Japan.
【本研究は生活習慣病の改善において患者自身による自分の医学データを認識することの意義を検討することを目的とした。702名の患者を対象にアンケート調査を行い,身体データ,生化学データ,指導摂取カロリー値に関して『次の項目の値を知っていますか』という質問に『はい』と答えた数を合計して病態認識度とした。6ヶ月後に患者の担当内科医師が病態改善度を評価し,患者認識度との関連を解析した。体重,腹囲,血圧,総コレステロール,HDLコレステロール,トリグリセリド,グルコース,HbA1c,摂取カロリーの項目値を認識する患者群の改善度は,それぞれ認識していない患者群の改善度に比較して有意に増加した。認識度が男性3以上および女性5以上の患者の改善度は,認識度1,2の男性と女性の対象の改善度よりそれぞれ有意に高値だった。多変量解析により,全項目の中で腹囲と血圧が,生化学データの中でHbA1cとHDLコレステロールが,身体および指導データの中で摂取カロリーと血圧が病態改善度と有意に関連した。以上の結果から,患者自身により自分の医学データを認識することが生活習慣病の病態を改善することに貢献する可能性が考えられる。
1) Department of Clinical Cell Biology, Chiba University Graduate School of Medicine, Chiba 260-8670.
2) Department of Genome Research and Clinical Application, Chiba University Graduate School of Medicine, Chiba 260-8670.
3) Toho University Sakura Medical Center, Sakura 285-8741.
4)Kimitsu Chuo Hospital, Kisarazu 292-8535.
5)Kuniyoshi Hospital, Isumi 298-0123.
6)Chiba Cardiovascular Center, Ichihara 290-0512.
7)Matsudo City Hospital, Matsudo 271-8511.
8)Omigawa General Hospital, Katori 289-0332.
ネフ由紀子1),武城英明2),宮下 洋3),内田大学4),伴 俊明5),田代 淳6,7),山崎健也7),石川 耕8),徳山隆弘8),姜 美子2),河村 徹2),齋藤 康1): 生活習慣病診療における患者が自分自身の医学データを認識することの役割.
1) 千葉大学大学院医学研究院細胞治療学,2) 千葉大学大学院医学研究院臨床遺伝子応用医学,3) 東邦大学医療センター佐倉病院,4) 君津中央病院,5) 国保国吉病院,6) 千葉県循環器病センター,7) 松戸市立病院,8)国保小見川総合病院
Tel. 043-226-2091. Fax. 043-226-2095. E-mail: hbujo@faculty.chiba-u.jp
2008年12月11日受付,2009年1月23日受理.
