




Volume 85, Number 4
doi:10.20776/S03035476-85-4-P169
[Original Paper]
Yumi Asano1), Ichiro Shimoyama2) and Atsushi Murata1)
(Received December 25, 2008, Accepted March 18, 2009)
Postural control in standing balance was analyzed in 80 volunteers, aged 31 to 92 years, who were free from equilibrium disease. Center of foot pressure (COP) was measured on a horizontal plane and in a vertical direction, during 20 sec with eyes open and 20 sec with eyes closed. COP-path length and COP-path area were obtained on the horizontal plane, and coefficient of correlation was tested for them with age, body weight and height. Integrated power between 0 and 10 Hz was tested for the horizontal medial-lateral oscillation, horizontal anterior-posterior oscillation, and vertical oscillation. Age was correlated with COP-path length and COP-path area, but body weight and height were not correlated with them. Age was correlated with the powers in the medial-lateral oscillation with eyes open and closed, and in the anterior-posterior oscillation with eyes closed. Body weight and height were correlated with the powers in the anterior-posterior oscillation with eyes closed and in the vertical oscillation with eyes open and closed. Conclusively, vision was important to the postural control for aged people, and the medial-lateral oscillation might increase with aging. Vertical oscillation correlated to body weight and height, which suggests important weight control for aged people.
vertigo, postural control, aging, center of foot pressure, vertical direction
Vertigo, dizziness and giddiness are one of frequent complaints met in home doctors, and the sensation of vertigo occurs so frequent especially for aged people. In home doctors, most of the patients with vertiginous complaints were consulted to a nearest otologist or neurologist, or were to start medical therapy without an established diagnosis. Major vertigious patients were far from serious pathology like as acoustic tumor, cerebellar infarction or bleeding[1], and minor patients were diagnosed as Ménière disease[2], vestibular neuronitis, or benign paroxysmal positional nystagmus[3]. Most vertigious patients have smooth prognosis with the conservative therapy of medication. Aged people are known to show declines in postural control during not only walking but also standing[4-5]. And accidental falls sometime cause aged people serious outcomes[6-7]. Many studies about postural control for aged people had reported a comparison between aged and young groups[8-11]. And, most of the reports had discussed about the postural control only on a horizontal plane. We studied postural control for aged people in a vertical direction and on a horizontal plane, by testing the coefficient correlations among age, body weight (BW), body height (BH) and the postural control.
Eighty volunteers, non vertigious patients who had been medicated for hypertension or hypercholesterolemia, were participated in this study. Informed consent was obtained from all subjects after fully explanation of this study. Mean age was 70 years and standard deviation was 11.5 (62 females and 18 males). They had no past history of vestibular diseases such as Ménière’s syndrome, vestibulitis syndrome, nor benign paroxysmal positioning vertigo. Mean BW was 56 Kg (standard deviation; ±10.4), and mean BH was 155 cm (±8.0cm).
Center of foot pressure (COP) was studied as for postural control, which was measured on a foot plate with 3 load cells[12]. Three signals from the cells were sampled at 20 Hz into 12 bit, and they were transformed into 3 signals; 2 were on a horizontal plane and one was in a vertical direction. COP-oscillations in the medial-lateral (M-L) and anterior-posterior (A-P) directions were studied on a horizontal plane, and those in the vertical direction were studied as a signal summed with the 3 load cells. Path length and path area of COP were studied on the horizontal plane. The path area was calculated with 2 shifts and a mean of COP-shifts on the horizontal plane.
Simple 2 tasks were asked to the subjects; one was to stand upright on the plate quietly with eyes open for 20 sec, and another was to do with eyes closed for 20 sec.
Power spectra of the oscillatory signals for each task were obtained with the fast Fourier transform for the M-L, A-P and vertical directions. Total powers between zero and 10 Hz were tested with the analysis of variance for the effects of the 3 directions and the 2 tasks, and the Bonferroni test was done for a post-hoc test.
The coefficient of correlations was obtained each other among COP-path length/sec, COP-path area/sec, age, BW, and BH. And the Spearman’s test was used to study significant correlations for further discussion.
Figure 1(Fig. 1) showed COP-dynamics on the horizontal plane for 2 cases of 50 and 86 years old females. Both subjects showed COP-oscillations increased with eyes closed (thin traces). The subject of 86 years showed marked oscillation with eye closed (thin trace at the right graph).
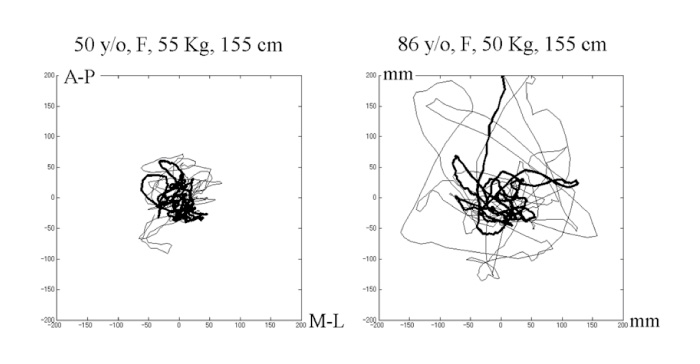
Fig. 1
COP-oscillation on a horizontal plane for typical 2 subjects of 50 and 86 years, with eyes open (thick trace) and with eyes closed (thin trace). The ordinate represented an anterior-posterior direction and the abscissa represented an medial-lateral direction in mm.
Figure 2(Fig. 2) showed the time course of the signals for the same subjects as in Fig. 1. The oscillations with eyes open showed fairly stable but those with eyes closed showed increased, which were noted for the signals from the 3 load cells, M-L direction, A-P direction, and the vertical direction. Mean path length was 114 mm/s (standard deviation; ±42.5) with eyes open, 227 mm/s (±90.3) with eyes closed, for all subjects. Mean area was 1555 mm2/s (standard deviation; ±981.6) with eyes open, 5078 mm2/s (±3608.9) with eyes closed, for all subjects. The correlation coefficient was 0.39 (P<0.05) between age and the path length with eyes open, was 0.37 (P<0.05) between age and path length with eyes closed, was 0.36 (P<0.05) between age and the path area with eyes open, and was 0.32 (P<0.05) between age and path area with eyes closed. Figure 3(Fig. 3) showed all data with age and their regression lines. The correlation coefficient was 0.34 (P<0.05) between the total power (0-10 Hz) of M-L shift and age with eyes open, and was 0.25 (P<0.05) between the total power of M-L shift and age with eyes closed, was not significant between the total power (0-10 Hz) of A-P shift and age with eyes open, and was 0.26(P<0.05) between the total power of A-P shift and age with eyes closed.
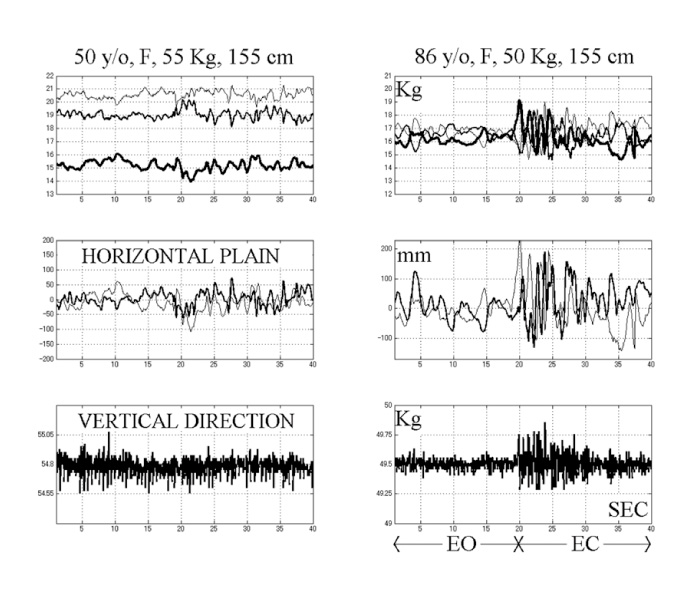
Fig. 2
COP-oscillations of the 2 subjects from the 3 load cells (2 upper graphs), M-L oscillation (thick trace) and A-P oscillation (thin trace) for the middle 2 graphs, and the vertical oscillation for the lower graphs. The abscissa represented the time course in second, the anterior half for the oscillation with eyes open and the posterior half for the oscillation with eyes closed. EO: with eyes open, EC: eyes closed.
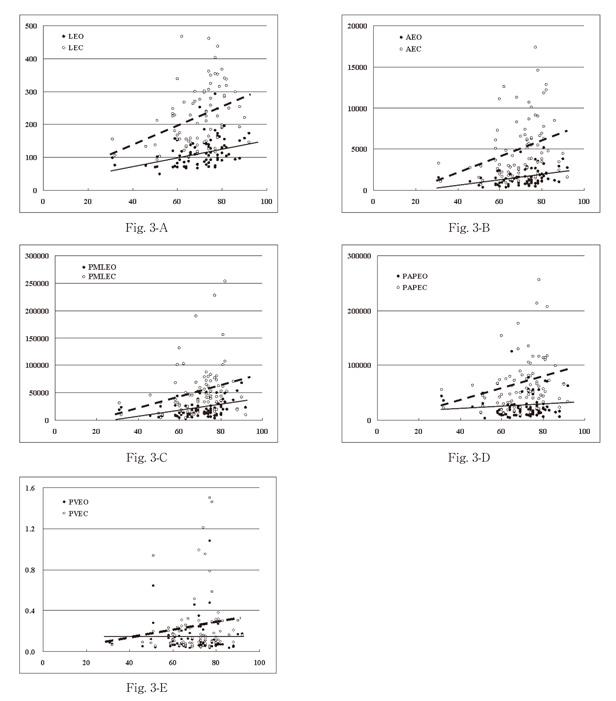
Fig. 3
Fig. 3-A showed the path length and age. A line was regression for the path length with eyes open, and a broken line was regression for the path length with eyes closed. (LEO: path length with eyes open, LEC: path length with eyes closed) Fig. 3-B showed the path area and age. A line was regression for the path area with eyes open, and a broken line was regression for the path area with eyes closed. (AEO: path area with eyes open, AEC: path area with eyes closed) Fig. 3-C showed the power in the M-L direction and age. A line was regression for M-L power with eyes open, and a broken line was regression for M-L power with eyes closed. (PMLEO: M-L power with eyes open, PMLEC: M-L power with eyes closed) Fig. 3-D showed the power in the A-P direction and age. A line was regression for A-P power with eyes open, and a broken line was regression for A-P power with eyes closed. (PAPEO: A-P power with eyes open, PAPEC: A-P power with eyes closed) Fig. 3-E showed the vertical power and age. A line was regression for vertical power with eyes open, and a broken line was regression for vertical power with eyes closed. (PVEO: vertical power with eyes open, PVEC: vertical power with eyes closed)
Figure 4 (Fig. 4)showed power spectra for the 3 directions of the same subjects as in Fig. 1 and 2. The power spectra with eyes closed showed increased on the horizontal plane for both subjects. For the vertical direction, the power spectra with eyes closed had increased for the subject of 86 years. But power spectra with eyes closed did not increase for the subject of 50 years. The analysis of variance was done for all subjects to show significant differences among the total powers for the effects of the 3 directions (P<0.0001) and of the 2 tasks (P<0.0001). The post-hoc test showed significant between the powers in M-L and A-P directions (P<0.003), between the powers in M-L and vertical directions (P<0.0001), and between the powers in A-P and vertical directions (P<0.0001).
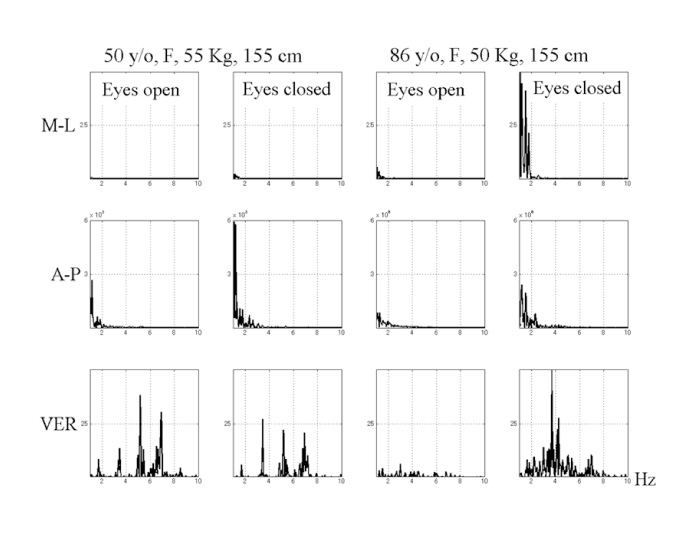
Fig. 4
Power spectra of the medial-lateral (M-L) direction (upper 4 graphs), the anterior-posterior (A-P) direction (middle 4 graphs), and vertical (VER) direction (lower 4 graphs), for the same subjects as in Fig. 1 and 2. The abscissa represented frequency (Hz). The ordinate represented power, and the dimension was all adjusted same as for all the directions.
Table 1 (Table 1) was a matrix of the coefficient of correlations for the total power of the oscillations. Significant correlations were noted between age and BH, between age and M-L power with eyes open, between age and M-L power with eyes closed, and between age and A-P power with eyes closed. Significant correlations were noted between BH and BW, between BH and A-P power with eyes closed, between BH and the vertical powers. Significant correlations were noted between BW and A-P power with eyes closed, between BW and the vertical powers. Significant correlations were noted between M-L powers with eyes open and those with eyes closed, between M-L powers with eyes open and A-P powers. Significant correlations were noted between M-L powers with eyes closed and A-P powers with eye closed, between M-L powers with eyes closed and the vertical powers with eyes closed. A significant correlation was noted between A-P powers with eyes closed and the vertical powers with eyes closed. A significant correlation was noted between the vertical powers with eyes open and the vertical powers with eyes closed.
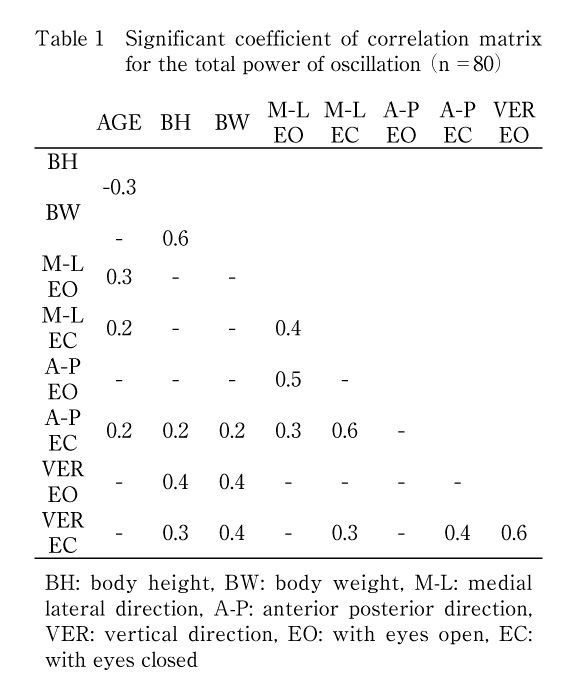
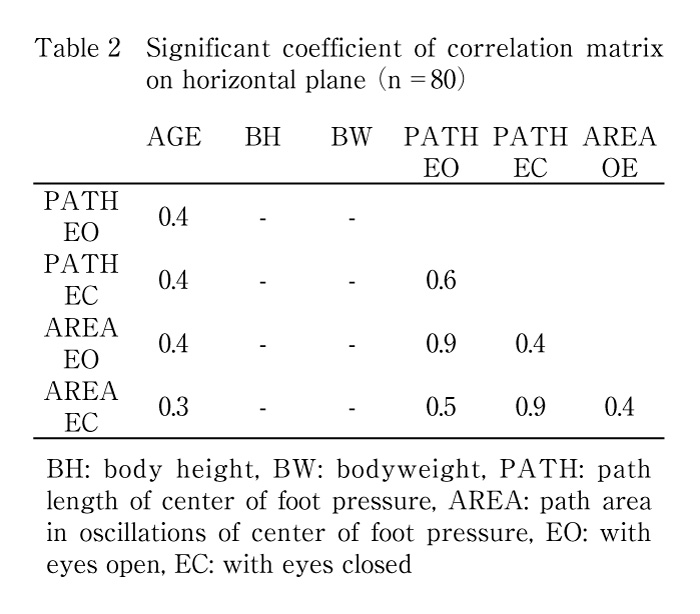
Table 2 (Table 2) showed a matrix of coefficient of correlations for the shifts on the horizontal plane, among COP-path length/sec, COP-path area/sec, age, BH and BW. The length and the area were correlated to age significantly, but not correlated to BH and BW.
Age was correlated to the total powers of the oscillatory signals in M-L direction with eyes open and closed. Age was correlated to the total powers with eyes closed in A-P direction.
The total powers in the vertical direction correlated to BH and BW, but did not correlate to age. Previous our study had shown spectra powers around 6 Hz in the vertical direction increased in proportion to aging[13]. In this study, the vertical oscillation showed no correlation to aging, but careful inspection of all individual data showed an inclination of the powers increased around 6Hz with aging. Therefore, the vertical oscillation shall be left for further study.
Age correlated to COP-path length and area on the horizontal plane. But BH and BW did not correlated to the length and area on the horizontal plane. Hue et al. had reported that body weight was a strong predictor of postural stability[14]. But, BW and BH correlated to the total powers in the vertical direction, which suggested both factors might be risk factors for aged falls from our results.
Standing upright is a complex multisensory function[15-16], using sensory-motor feedback from vestibular[17], visual[18-19], auditory[20], proprioceptive[18]and somatosensory systems [21].
Aging is an ultimate problem for humans, and aging might be one of frequent explanations to vertigious patients. But precise diagnosis might provide us appropriate order-made therapy.
An occasional aged patient complained of lasting dizziness sensation with conservative medication, who had diagnosed as no marked equilibrium disease by otologists. For any cases, dizziness sensation should be considered as side effects from medicines for other disorders. When COP-path length and area were within normal range for his/her age, the vertical oscillation should be measured. And other specialists might be consulted, e. g., neurologists, ophthalmologists, endocrinologists, psychologists and so on.
In conclusion, this simple non-invasive COP-measurement in the vertical and horizontal directions, will provide more information as objective and quantitative data to us and patients. Precise evaluation, chronological course, effects of medical therapy, and effects of rehabilitation will be provided for postural control.
We thank all the subjects and Yukinobu Kobayashi MD, PhD for clinical evaluation of patients, and for his constant support.
日常多く遭遇する高齢者の眩暈・眩暈感・浮遊感は加齢現象と処理され十分解明されていない。高血圧または高脂血症にて通院中の31歳から92歳までの80名のボランティアから研究の趣旨を説明後,同意を得て静止立位の足圧中心を記録解析し,年齢・体重・身長と姿勢制御機能の相関を検討した。被検者の平均体重は56Kg(標準偏差±10.4)で,平均身長は155㎝(±8.0)で,既往歴にメニエール・前庭神経炎・良性頭位変換眩暈はない。3ロードセルで支持した足底板に載り20秒の開眼静止起立位と20秒の閉眼静止立位を施行した。3荷重を20Hz,12bitで収集し水平面内前後方向・左右側方と,鉛直方向の信号とした。水平面内の足圧中心の移動距離と移動面積と,フーリエ解析によるパワーを前後方向・左右側方と鉛直方向について求め0~10Hzまでの積分値として,年齢・体重・身長との相関係数を求めスピアマン検定により有意な係数を検討した。移動距離・面積ともに開眼・閉眼時に年齢と有意に相関が認められた。移動距離・面積とも身長・体重とは無相関であった。パワー値との相関で年齢との間に有意相関が認められたのは開眼閉眼とも左右側方と閉眼時の前後方向との間で,身長との相関では閉眼時前後方向と開閉眼時の鉛直方向との間に有意相関が認められた。体重との相関でも閉眼時前後方向と開閉眼時の鉛直方向との間に有意が認められたが,これらの結果は視覚機能が反映したものと推測した。今後,運動感覚機能低下のみならず,足圧中心変動は少ないのに眩暈感を訴える症例などの高次認知機能をも考慮した眩暈感の原因を詳細に検討し,転倒防止・予防に応用したい。
1) Department of Rehabilitation, University Hospital, Chiba University, Chiba 260-8677.
2) Section for Human Neurophysiology, Research Center for Frontier Medical Engineering, Chiba University, Chiba 263-8522.
浅野由美1), 下山一郎2), 村田 淳1): 静的姿勢制御機能における加齢変化-鉛直・水平方向の足圧中心振動と年齢・体重・身長-.
1) 千葉大学医学部附属病院リハビリテーション部, 2) 千葉大学フロンティアメディカル工学研究開発センター脳機能計測解析研究部門
Tel. 043-226-2620. Fax. 043-226-2338. E-mail: asayumi@faculty.chiba-u.jp
2008年12月25日受付,2009年3月18日受理.
