




Volume 85, Number 4
doi:10.20776/S03035476-85-4-P185
[Case Report]
Junichi Nakamura1), Yutaka Ono2) , Akira Ogasawara
2)
Shunji Kishida1), Koya Kamikawa3) and Kazuhisa Takahashi1)
(Received February 23, 2009, Accepted March 18, 2009)
As life expectancy rises, the number of elderly patients who are potential candidates for surgery is also increasing rapidly. We reported the eldest male patient, who was 107-year-old, with femoral intertrochanteric fracture that we have managed with osteosynthesis under spinal anaesthesisa. The fracture was classified as type 1, group 3 under the Evans’s classification and was fixed with a compression hip screw. The patient was able to walk with the assistance of a nurse without pain after surgery. He died from pneumonia 11 months later. Our experience suggests that surgery for hip fractures in centenarians poses a challenge; successfully meeting this challenge requires optimal anaesthesia.
Centenarian, Hip fracture, Femoral intertrochanteric fracture, osteosynthesis
In 2006, the population of centenarians in Japan increased to 29,000[1]. In United States, the centenarian population was approximately 81,000 in 2000; this population is projected to increase to 214,000 in 2020 and to exceed 800,000 by 2050[2]. As life expectancy rises, the number of elderly patients who are potential candidates for surgery is also increasing rapidly. For instance, the number of new cases with hip fracture in Japan increased from about 9,200 in 1997 to 110,000 in 2000 and is projected to rise to 220,000 in 2020 in Japan[3-4]. The indications for surgical treatment remain controversial in very elderly patients. We reported the eldest male patient with femoral intertrochanteric fracture that we have managed with surgical treatment. The patients and their families were informed that data from the case would be submitted for publication, and gave their consent.
The patient, a 107-year-old male, was referred to our hospital with a suspected femoral intertrochanteric fracture of his right hip, one day after he had fallen in the dining room of a nursing home. The patient had had a high degree of independence in his activities of daily living before injury, including being able to walk without a cane.
The patient’s medical history included a femoral intertrochanteric fracture of his left hip, treated conservatively at another hospital two years earlier. He also had suffered from two incidents of pneumonia: one three years before and the other two months before his right intertrochanteric fracture.
Physical examination demonstrated severe pain and deformity of the right hip, but peroneal nerve palsy was not observed.
An anteroposterior plain radiograph of the pelvis revealed a displaced femoral intertrochanteric fracture of the right hip (Fig. 1). No residual deformity from the left hip fracture was noted. Following unsuccessful efforts to reduce the fracture, characterized by persistent displacement of the lesser trochanter and medial cortex and instability under direct traction of 4kg, the patient’s fracture was classified as type 1, group 3 under the Evans’s classification (Fig. 2a) [5].

Fig. 1
Admission anteroposterior radiograph of the pelvis
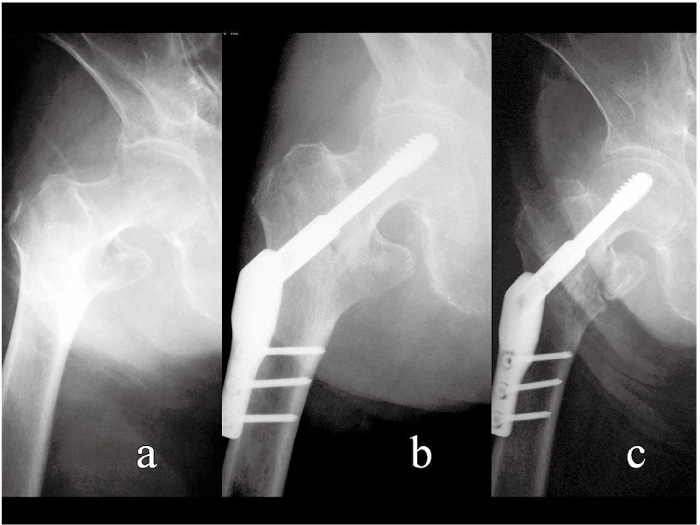
Fig. 2
Anteroposterior radiograph of the right hip
(a)Direct traction of 4kg was unsuccessful in reducing the fracture, leaving a persistent displacement of the lesser trochanter and medial cortex of the calcar. This response indicates an unstable fracture, classified as Type 1 Group 3 under the Evans classification.
(b)Postoperative x-ray shows acceptable repositioning.
(c)X-ray six months later demonstrates bone healing of the intertrochanteric fracture.
Ventricular extrasystoles and negative T waves were observed in an electrocardiogram. Blood gas analysis showed pH 7.52, PaCo2 31.7mmHg, PaO2 67.7mmHg, and arterial oxygen saturation (SaO2) 96%. Blood chemistry testing showed anemia (hemoglobin (Hb) 12.6g/dl), thrombocytopenia (11.2×104/μl), hypoproteinemia (total protein 6.3g/dl, albumin 3.8g/dl), hyperbilirubinemia (total bilirubin 1.8mg/dl, direct bilirubin 0.5mg/dl), and hyponatremia (Na 134mmol/l). The patient and his family requested surgical treatment even though the risk of operation was considered to be extremely high.
The operation was performed under spinal anesthesia three days after admission. 1.4ml of 0.5% Bupivacaine (Marcain) was injected between the third and forth lumbar vertebrae.Ten minutes later, tachycardia and hypoxemia were observed, but blood pressure was maintained and SaO2 recovered following the administration of O2 4L (40%) via a Venturi mask. Open reduction and internal fixation of the hip fracture was achieved with a compression hip screw (Best Medical, Saitama, Japan), 135 degrees with 3 holes (Fig. 2b). Operative time was 25 minutes.
Blood transfusion (2 units) was needed to correct the patient’s anemia (Hb 9.6g/dl) after surgery. To maintain an in-out urinary balance, furosemide (lasix) 10mg/day was prescribed for oliguria (<20ml/hr). Transfer to a wheelchair began the next day. The patient was able to walk to-and-fro using parallel bars and he returned to the nursing home seven days after surgery. He was able to walk with the assistance of a nurse without pain six months later. (Fig. 2c) The patient died from pneumonia 11 months after his surgery.
To our knowledge, this 107-year-old patient is one of the oldest males in the world who have undergone osteosynthesis for femoral intertrochanteric fracture. Sakamoto et al.’s survey of 10,992 hip fractures in Japan included one 111-year-old patient, who survived over one year after fracture; the survey, however, did not provide any information about the patient’s sex, fracture type, and treatment[6]. Forster et al. also included the case of a 107-year-old patient in their report on proximal femoral fracture, but provided no further details[7]. Warner et al. described performance of an emergency arthroplasty in a 107-year-old woman, but did not list her diagnosis[8]. Konttinen et al. reported three 102-year-old patients (one male and two female) with femoral intertrochanteric fractures treated with osteosynthesis[6]. Katlic et al. reported two 100-year-old patients who underwent osteosynthesis for femoral intertrochanteric fractures and hemiarthroplasty for femoral neck fractures[5]. Thus, among these studies, the oldest male patient with a detailed description of osteosynthesis for femoral intertrochanteric fracture was 107 years of age.
Zuckerman et al. reported a mortality rate among elderly patients ranging from 14% to 36% one year after hip fracture; approximately 50%-65% of patients regained their previous level of ambulation, 10%-15% were limited to household ambulation, and up to 20% became nonambulatory[9]. Forster et al. reported that 13 centenarians with proximal femur fractures had cumulative mortalities at 30 days, 6 months, and 1 year of 31%, 50%, and 56%, respectively[8]. Similarly, Konttinen et al. reported that 12 centenarians undergoing emergency surgery had cumulative mortalities after 30 days, 6 months and 1 year of 25%, 42%, and 50%, respectively[10]. These high mortality rates reported after operations in centenarians do not necessarily indicate that surgeries in centenarians have poor outcomes, because centenarians overall have a short life expectancy (less than two years)[9-11]. Zuckerman et al. suggested that mortality rate for centenarians after surgery was almost same as the mortality rate from natural courses[9].
Katlic et al. described two 100-year-old women who lived over two years postoperatively and advised that centenarians should not be denied emergency surgery simply because of their chronologic age[11]. A 2004 Japanese survey found that 94% of patients with femoral trochanteric fractures were treated surgically[4]. Konttinen et al. also stated that centenarians tolerated anaesthesia and surgery quite well when serious efforts were made to maintain haemodynamic stability during anaesthesia[10]. Moran et al. reported that mortality after hip fracture did not increase when surgery was delayed up to three days; however, a delay of four or more days significantly increased mortality[12]. In our patient, the interval from fracture to admission was one day and the duration from admission to surgery was three days, compared with average values from a Japanese survey of 3.1 days to admission and 11.2 days to surgery[6].
The treatment of hip fractures in centenarians poses a challenge. Although the risks of anesthesia and surgery are extremely high, centenarians may have the most to benefit from surgical treatment. Immobilization in the very elderly is poorly tolerated and may quickly cause social and physical morbidity or even death. Fukushima et al. reported that contralateral hip fractures occurred within five years in more than 70% of patients with hip fractures[13]. Our patient and his family were more satisfied with outcome of surgical treatment for this hip fracture than they were with the outcome of the conservative management of his previous contralateral hip fracture.
The perioperative period is the most vulnerable time. Optimal anaesthesia, expeditious surgery and a coordinated multidisciplinary approach to care are essential. Regarding the type of anaesthesia, Sutcliffe et al.’s study of 1,333 hip fracture cases found that spinal and general anaesthesia were equally safe, and the authors expressed a preference for spinal anaesthesia in patients with pulmonary disease[14]. Konttinen et al.’s study findings suggested that the total amount of intrathecal local anaesthetic required was significantly less in elderly patients than the amount required for similar surgery in middle-aged patients[10]. In elderly patients, hypotension commonly occurred secondary to hypovolemia and dehydration, while excessive transfusions caused heart failure. The Hb trigger point for transfusion ranged from 8.0 to 10.0 g/dl.
In conclusion, this 107-year-old patient is the oldest male patient in whom we have performed osteosynthesis for femoral intertrochanteric fracture. Our experience suggests that surgery for hip fractures in centenarians poses a challenge; successfully meeting this challenge requires optimal anaesthesia.
高齢化社会を迎えて,大腿骨頚部/転子部骨折患者の受傷時年齢も年々超高齢化しており,しばしば治療法の選択について苦慮することがある。大腿骨転子部骨折の手術例としては世界最高齢と思われる,107歳男性を経験したので報告する。骨折型はEvans分類Type 1 group 3の不安定型骨折で腰椎麻酔下に骨接合術を施行した。疼痛なく介助歩行可能となったが,術後11カ月後に肺炎で死亡した。100歳以上の患者は周術期管理に注意を要するが,手術により早期離床が可能であると思われた。
1) Department of Orthopaedic Surgery, Graduate school of Medicine, Chiba University, Chiba 260-8677.
2) Department of Orthopaedic Surgery, Chosei Public Hospital, Mobara 299-4114.
3) Department of Orthopaedic Surgery, Teikyo University Chiba Medical Center, Ichihara 299-0111.
中村順一1),小野 豊2),小笠原 明2),岸田俊二1),神川康也3),高橋和久1): 107歳男性の大腿骨転子部骨折に対する骨接合術の1例.
1) 千葉大学大学院医学研究院整形外科学, 2) 公立長生病院整形外科, 3)帝京大学ちば総合医療センター整形外科
Tel. 043-226-2117. Fax. 043-226-2116. E-mail: njonedr@yahoo.co.jp.
2009年2月23日受付,2009年3月18日受理.
