




Volume 85, Number 5
doi:10.20776/S03035476-85-5-P241
[Original Paper]
Yumi Asano1), Ichiro Shimoyama2) and Atsushi Murata1)
(Received December 25, 2008, Accepted March 18, 2009)
Measuring center of foot pressure (COP) in motion might be more useful than only doing static COP to evaluate postural control. Active knees movements were applied to study COP with aging. Shifts and oscillation of COP were discussed in relation to age, body weight and height for 95 volunteers. Informed consent was obtained from them after fully explanation about this study. They had no past history of vestibular diseases. The subjects on a force plate were asked to stand upright for 5 sec, flex knees at an angle about 90 degrees as they could and keep knees flexed for 9.5 sec and extend knees to stand upright for 5 sec. Vertical, medial-lateral, anterior-posterior COP were tested. Medial-lateral shifts significantly correlated to age, and medial-lateral oscillation increased with aging. Anterior-posterior shifts in flexing knees correlated negatively to age, but anterior-posterior shifts at knees flexed correlated positively to age. Vertical shifts did not correlate to age, but they correlated to weight both in flexing and flexed knees, and anterior-posterior shifts correlated to weight in flexing knees. Both vertical and anterior-posterior shifts correlated to height in flexing knees. COP shifted anterior in knee-flexion. Oscillation about 2 Hz increased during flexed knees in the vertical direction.
postural control, dynamic, aging, center of foot pressure, knee flexion
COP; center of foot pressure, M-L; medial-lateral, A-P; anterior-posterior
Postural control had been discussed in a standing posture by major reports[1-3]. But postural control is not so simple as to elucidate the mechanism with only studying the posture in standing upright quietly. Then turbulence has been applied to the standing posture, some power was suddenly administered from the outside to a subject, e. g., on a sudden moving platform[4,5]or tugging or pulling subjects at the waist[6]. Those methods, in applying turbulence, were a kind of passive and reflex-like movements, so the method is occasionally hard to test for aged people. Active movements were other methods to study postural control[7-9], which were all active and voluntary movements.
We studied dynamic postural control with aging during active voluntary movements; flexing knees moderately, keeping the knees flexed at the angle and extending knees. We measured shifts and oscillation of a center of foot pressure (COP) in a vertical direction and on a horizontal plane.
Ninety five volunteers, who had been medicated for hypertension or hypercholesterolemia, participated in this study. Informed consent was obtained from every subject after fully explanation about this study. Mean age was 70.7 years (standard deviation; ±11.0), aged 31 to 92 years (74 females and 21 males). They had no past history of vestibular diseases such as Ménière’s syndrome, vestibulitis syndrome, nor benign paroxysmal positioning vertigo. Mean body weight (BW) was 56.3 Kg (±10.3) from 33 to 91.5 Kg, and mean body height (BH) was 154.8 cm (±8.0) from 136 to 173 cm.
Center of foot pressure (COP) was measured with the same force platform as that in the previous study[10-11]. Shortly, the subject was asked to stand on a plate with 3 load cells, and the 3 force signals were sampled at 20 Hz into 12 bit to be converted into oscillations in a vertical, medial-lateral(M-L), anterior-posterior (A-P) and vertical directions for further discussion.
The subjects were asked to stand upright quietly on the force platform with eyes open for 5 sec, then they were asked to flex knees around an angle of 90 degrees as possible as they could and keep the knee flexing for 9.5 sec, and asked to extend knees to stand upright for 5 sec.
Maximum COP shifts during each task were measured for M-L, A-P, and vertical oscillations; the shift during standing upright, the shift during knees flexion, and the shift during knees extension. The maximum shift during knees flexion (9.5 sec) was for flexing motion, and the maximum shift during the last 5 sec was for a shift at flexed knees. Then, the shifts were normalized with the shift during standing upright, for further statistical tests. Power spectra of the oscillatory signals for each task were obtained with the fast Fourier transform for the vertical, M-L, and A-P directions. Mean power for every 2 Hz were tested with the analysis of variance for the effects of the 3 directions and the 3 tasks, and the Bonferroni test was done for a post-hoc test.
The coefficient of correlation was obtained with each other among COP-shifts during the tasks, age, BW, and BH. And the Spearman’s test was used to study significant correlations for further discussion.
Figure 1(Fig. 1) showed dynamics of COP in flexing and extending knees on the horizontal plane for a male of 60 years. COP moved anterior during knees flexion (a thin plot) and COP moved back posterior during knees extension (dotted plots). Shifts on knees flexed (anterior part of a thin plot) showed much oscillation than shifts in standing upright (posterior part of a thick plot).
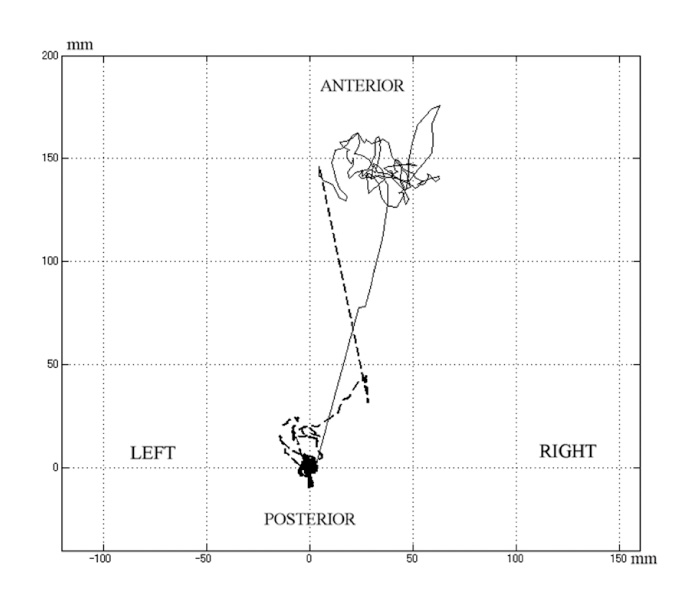
Fig. 1
Dynamic COP during knees flexion for a male of 60 years on a horizontal plane. A thin plot was for knees flexion, dotted plots was for knees extension, and standing upright was for a thick plot. The ordinate represented anterior-posterior direction and the abscissa did medial-lateral direction in mm.
Figure 2(Fig. 2) showed the shifts in the time course of M-L, A-P and vertical directions for the same subjects as in Fig. 1. Oscillations and shifts were noted stable at the early 5 sec during standing upright, and shifts and oscillations increased at the middle 19.5 sec during knees flexion, and oscillations and shifts showed moderate at the last 5 sec during knees extension. Oscillations and shifts were noted for all directions. Oscillations and shifts in A-P direction showed larger than those in M-L direction during knees flexion.
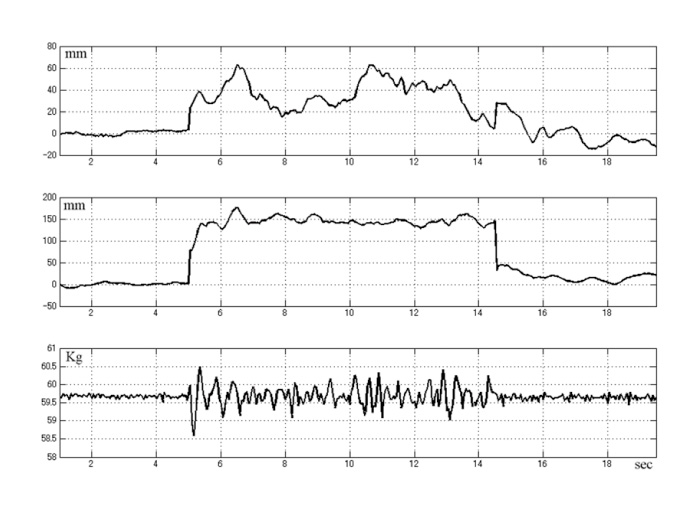
Fig. 2
Medial-lateral (upper), anterior-posterior (middle) and vertical (lower) oscillations for a male of 60 years. The ordinate represented shifts of COP in mm for medial-lateral and anterior-posterior directions and in Kg for a vertical direction. The abscissa represented a time course in sec; standing upright for the early 5 sec, knees flexion for the middle 9.5 sec, and knees extension for the last 5 sec.
Figure 3(Fig. 3) showed oscillations and shifts for all subjects in a graph, oscillations and shifts showed inter-individual variation, but all subjects showed oscillations and shifts increased during knees flexion.
Coefficient correlations between the normalized maximum COP shifts and age were tested for each task, the shifts in A-P direction were negatively correlated to age during knees flexion (-0.50, P<0.05) and during knees extension (-0.27, P<0.05).
The young group under 65y/o showed significant much shift than the aged group over 66 y/o, tested with the normalized maximum COP shifts (P<0.05). The post-hoc test showed significant between groups in M-L and vertical directions (P<0.0001), and between groups in A-P and vertical directions (P<0.0001), and showed significant between groups during knees flexion and knees flexed (P<0.0001), and between groups during knees flexed and knees extension (P<0.0001).
Variances of mean signals for every 1 sec was tested among those during standing upright, knees flexion and knees extension with the analysis of variance. Variances of the mean oscillations showed significant differences among them (P<0.05). The post-hoc test showed significant between the variances during standing upright and those during knees flexion (P<0.0001), between those during standing upright and those during knees extension (P=0.016), and between those during knees flexion and those during knees extension (P<0.0001).
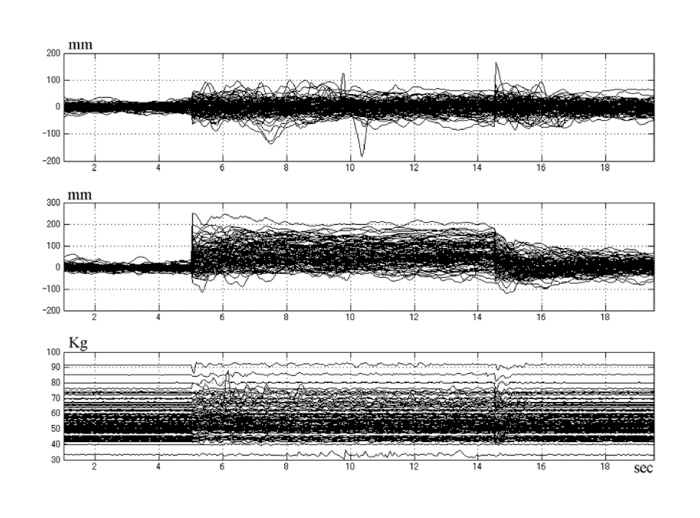
Fig. 3
Oscillations and shifts in medial-lateral (upper), anterior-posterior (middle) and vertical (lower) directions for all subjects. The ordinate represented shifts of COP in mm for medial-lateral and anterior-posterior directions, and in Kg for a vertical direction. The abscissa represented a time course in sec; standing upright for the early 5 sec, knees flexion for the middle 9.5 sec, and knees extension for the last 5 sec.
Figure 4(Fig. 4) , upper 9 graphs, showed power spectra for all subjects; those during 5 sec at standing upright, those during 9.5 sec at knees flexed, and those during 5 sec at knees extension. The powers, in the vertical direction, around 2 Hz at knees flexed showed remarkably increased, those around 5 Hz at knees extension showed fairly increased, and those around 6 Hz at standing upright showed fairly increased. The powers, in A-P direction, below 3 Hz at knees flexed showed moderate increased, those below 2 Hz at knees extension showed moderate increased, and those around 1 Hz at standing upright were noted. The powers, in M-L direction, below 5 Hz at knees flexed showed moderate increased, those below 3 Hz at knees extension showed moderate increased, and those below 2 Hz at standing upright were noted.
Mean powers for every 2 Hz were tested for the effects of the tasks and of the directions by the analysis of variance. Powers showed significant differences among the tasks and among directions (P<0.05).
Figure 4(Fig. 4) , lower 6 graphs, showed normalized power spectra with the power spectra at standing upright, respectively, for all subjects. The powers, in the vertical direction, around 2 Hz at knees flexed showed remarkably increased, but those at knees extension and those at standing upright did not show distinguishable increases. The powers showed no distinguishable increase in A-P and M-L directions.
Mean powers in dB for every 2 Hz was tested for the effects of the tasks and of the directions by the analysis of variance. The powers showed significant differences between the tasks (P<0.05). Then the student t-test showed the powers in the M-L and A-P directions no significant between knees flexed and extension. A significant difference was noted in the vertical direction between knees flexed and extension. Then 3 band powers between 0.5 and 3 Hz, between 3.5 and 7 Hz, and between 7.5 and 10 Hz, were tested for the effects of the tasks. The band power between 0.5 and 3 Hz was significantly high than the other bands (P<0.001). Peaks were noted around 2 Hz for knees flexed in the vertical direction.
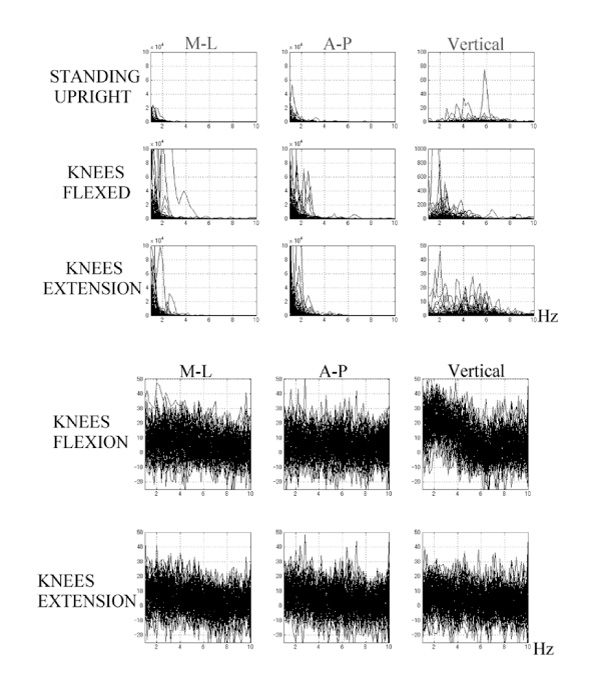
Fig. 4
Upper 9 graphs showed power spectra of COP oscillations for all subjects, during standing upright (upper 3 graphs), knees flexed (middle 3 graphs) and knees extension (lower 3 graphs). The left column showed spectra for a medial-lateral direction, the middle column showed spectra for an anterior-posterior direction, and the right column showed spectra for a vertical direction. The abscissa represented frequency in Hz, and the ordinate represented powers of the oscillations.
Lower 6 graphs showed normalized power spectra of COP oscillations during knees flexed (upper 3 graphs), and knees extension (lower 3 graphs) for all subjects. The left column showed the oscillations for medial-lateral direction, the middle column showed those for anterior-posterior direction, and the right column showed those for a vertical direction. The abscissa represented frequency in Hz, and the ordinate represented the powers of oscillations in dB.
Figure 5(Fig. 5), upper 3 graphs, showed grand mean power spectra of COP oscillations during standing upright, knees flexed and knees extension. The upper row of Fig. 5 was for power spectra and the lower row was for the normalized power spectra with powers at standing upright. The left column showed the oscillations for a M-L direction, the middle column showed those for an A-P direction, and the right column showed oscillations for a vertical direction. The abscissa represented frequency in Hz, and the ordinate represented powers of oscillations.
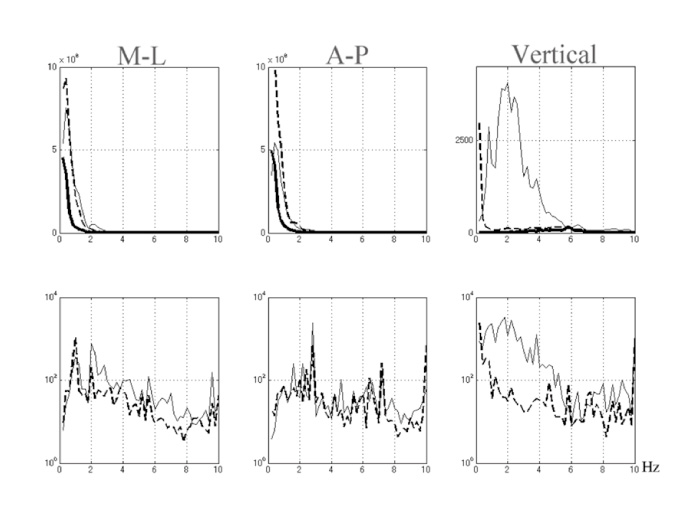
Fig. 5
Grand mean power spectra of COP oscillations during standing upright (thick plots for upper only), knees flexed (thin plots) and knees extension (dotted plots). The upper row was for power spectra and the lower row was for the normalized power spectra with powers at standing upright. The left column showed the oscillations for a M-L direction, the middle column showed those for an A-P direction, and the right column showed oscillations for a vertical direction. The abscissa represented frequency in Hz, and the ordinate represented powers of oscillations.
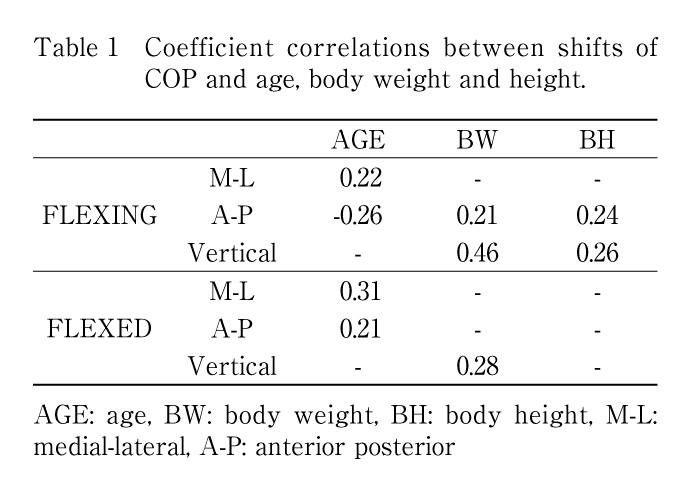
Table 1 (Table 1) was coefficient correlations between shifts of COP and age, body weight and height. Shifts of COP in flexing, those were measuring maximum shift from the beginning of the instruction until just before the beginning of the extension. Correlation was significant between M-L shifts and age, negative correlation was significant between A-P shifts and age. Correlation was significant between A-P shifts and body weight, and between the vertical shifts and body weight.
No significant correlation was noted between M-L shifts and body weight. Correlation was significant between A-P shifts and body height, and between the vertical shifts and body height. No significant correlation was noted between M-L shifts and body height. Shifts of COP in flexed, those were measuring maximum shift during holding knees flexed. Negative correlation was significant between A-P shift and age, and positive correlation was significant between the vertical shift and body weight. No significant correlation was noted between the shift and body height.
Medial-lateral shifts significantly correlated to age in the dynamic COP, i. e., M-L oscillation increased with aging. Anterior-posterior shifts on flexing knees correlated negatively to age, but A-P shifts at knees flexed correlated positively to age. Vertical shifts did not correlate to age in the dynamic COP. Vertical shifts correlated to BW both on flexing and flexed knees, and A-P shifts correlated to BW in flexing knees. Body height correlated to both vertical and A-P shifts in flexing knees. Flexing knees is a series of sequential movements; one is standing upright and moves knees, hip and ankle joints in collaboration with each other, and so many muscles coordinate each other around those joints. COP shifted anterior on the knees flexion in A-P direction. In flexing knees, acceleration, speed and shift were varied inter- and intra-individually, moreover, knees flexed were sometime hard for aged people. Pain around the joints and/or muscle weakness obstructs smooth movements, and affects knees stable. Therefore, only the instruction was the most we could for the aged outpatients to “flex your knees at around an angle of 90 degrees and hold them and extend them as you could, please”. Moderate knees flexion was indistinct and arbitrary, but the instruction was provided in the same way for all subjects. In measuring COP, longer recording for one task might be better for the diagnosis, but shorter recording is better for aged people. So, 9.5 sec was also compromised to keep knees flexed, following our previous unpublished study. Simultaneous recording of acceleration or motion picture would be helpful to normalize the shifts with the motion in the future study.
Postural control needs multi-sensory function [5,12] , using sensory-motor feedback from vestibular [13] , visual [14,15] , auditory [16] , proprioceptive [17] and somatosensory systems [18] . Therefore, static and dynamic COP might suggest a useful examination to evaluate above systems and monitor above systems in rehabilitation. Postural control have been reported to be useful for multiple sclerosis [19] , Spinal cord-injury [20] , stroke [20] , scoliosis [22] , Parkinson’s disease [23] , essential tremor [24] etc.
In conclusion, dynamic COP, in a vertical direction and on a horizontal plain, will provide us more information than only the static COP did for the postural control. M-L oscillations increased with aging by the dynamic COP. Anterior shifts increased with aging at knees flexed but decreased in flexing knees. Vertical shifts correlated to BW, but the shifts did not correlate to age for the dynamic COP. Vertical and A-P shifts correlated to BH in the dynamic COP. Dynamic COP provides us precise evaluation, chronological course, effects of medication and rehabilitation for the postural control. Standardizing COP with age, BW and BH should be a problem in future.
We thank all the subjects and Yukinobu Kobayashi MD, PhD for clinical evaluation of patients, and for his constant support.
日常外来における姿勢制御機能検査は直立起立位で開眼閉眼負荷をおこなう静的な検査で主流であったが,最近,ダイナミック姿勢制御について報告され始めた。研究所内でヒトの載った重心動揺計などの装置の角度を突然変化させるなど,立位健康人へ外乱を与える報告が多く,臨床における高齢者に施行するには困難な方法が多い。さらに受動的外乱が多く反射的な立ち直り機能を解析している。自から運動始める能動的運動によるダイナミック姿勢制御機能の報告は非常にすくない。膝屈曲伸展運動の報告はこれまで見当たらない。31から92歳(平均70.7標準偏差11.0)の高血圧・高コレステロール血症で内服加療中の95ボランティアから研究の趣旨を説明後,同意を得て,立位5秒→中腰位9.5秒→立位5秒の運動中の足底圧中心を計測し,その変位とスペクトル解析結果と,年齢・体重・身長との相関を検討した。課題は統一し「できる範囲で膝を90度くらいに曲げてください」とした。被検者の平均体重は56Kg(±10.3)で,平均身長は155㎝(±8.0)で,既往歴にメニエール・前庭神経炎・良性頭位変換眩暈はない。足底圧中心を水平面内前後方向・左右側方と,鉛直方向の信号として20Hz, 12bitで収集し。足圧中心の変位と,5秒間のフーリエ解析によるパワーの年齢・体重・身長との相関係数を求め,スピアマン検定で有意な係数を検討した。左右側方の変位は年齢に有意に相関して大きくなった。前後の変位は膝屈曲運動により年齢に相関して小さくなった。屈曲位保持時の揺れは年齢に相関して大きくなった。鉛直方向の揺れは年齢との相関は見られなかった。鉛直方向の揺れは体重と相関が認められ,膝屈曲運動では前後方向の揺れと体重にも相関が認められた。膝屈曲運動変位は身長は前後方向にも鉛直方向にも相関が認められた。膝屈曲位保持により水平面内の前後方向左右側方向に特徴的な周波数増加はみられないが,鉛直方向に2Hz付近の振動が増加した。静的のみならず動的負荷することにより多くの情報が得られ,リハビリテーションの評価などに応用したい。
1) Department of Rehabilitation, University Hospital, Chiba University, Chiba 260-8677.
2) Section for Human Neurophysiology, Research Center for Frontier Medical Engineering, Chiba University, Chiba 263-8522.
浅野由美1), 下山一郎2), 村田 淳1): 動的姿勢制御機能における加齢変化-立位から膝屈曲・屈曲保持・伸展-.
1) 千葉大学医学部附属病院リハビリテーション部, 2) 千葉大学フロンティアメディカル工学研究開発センター脳機能計測解析研究部門
Tel. 043-226-2620. Fax. 043-226-2338. E-mail: asayumi@faculty.chiba-u.jp
2008年12月25日受付,2009年3月18日受理.
