




Volume 86, Number 1
doi:10.20776/S03035476-86-1-P1
[Case Report]
Takeshi Yamaguchi, Seiji Ohtori, Masaomi Yamashita, Takana Koshi, Kazuyo Yamauchi Chikato Mannoji, Munetaka Suzuki, Hidetaka Higashi, Tamio Kon Akira Hirose, Masashi Takaso, Yasuchika Aoki, Gen Inoue and Kazuhisa Takahashi
(Received September 8, 2009, Accepted September 30, 2009)
A 60-year-old patient presented with a six-month history of severe sciatica. The patient showed tenderness of Valleix and Friberg’s sign, and his symptoms disappeared after injection of lidocaine both onto the sciatic nerve and onto the L5 spinal nerve. MRI revealed left extraforaminal disc herniation at the L5/S1 level and thickness of the piriformis muscle. The symptoms did not improve after conservative treatment; second stage surgery was performed under a diagnosis of double lesion neuropathy at the lumbar spine and at the piriformis muscle. For release of sciatic nerve compression, incision of the piriformis muscle was performed. The symptoms decreased; however, they persisted. Surgical treatment for the lumbar lesion was performed. The symptoms disappeared immediately after surgical removal of the disc herniation and posterolateral fusion. It is important to consider double crush syndrome at lumbar lesion and piriformis levels.
piriformis syndrome, sciatica, lumbar, disc herniation, surgery
Originally described by Robinson in 1947, piriformis syndrome (PS) is a constellation of symptoms that include low back or buttock pain referred to the leg [1]. It is estimated that at least 6% of patients who are diagnosed as having low back pain actually have piriformis syndrome [2-4].
Some authors have reported that the peripheral nerve is compressed at two sites, known as double crushed neuropathy. The most common sites were the cervical spine, the cubital tunnel at the elbow joint, and the carpal tunnel at the wrist joint [5-7]. However, there has been no reported case of sciatica, which is caused by compression from both a lumbar disorder and from the piriformis muscle.
Here we report a rare case of sciatica in a 60-year-old man, which is caused by compression from a lateral L5/S1 intervertebral disc herniation and from the piriformis muscle.
The protocol for human procedures used in this study was approved by our institution’s ethics committee. This report was also approved by the patient after informed consent. A 60-year-old man presented with a six-month history of left sciatica involving the left lower extremities. He presented at our hospital in 2005 with complaints of pain in his buttocks and the lateral aspects of his legs. There was apparent motor weakness of left extensor hallucis longus (Manual Muscle Test: MMT 4/5). Sensory examination confirmed left hypoalgesia in the lateral aspect of his lower legs corresponding to the L5 dermatome. On the left side, a straight leg raising test was negative, Friberg (hip joint external rotation test), and Pace (flexion, adduction, and internal rotation test) tests were positive. He demonstrated severe tenderness of Valleix in the buttock area.
Plain X-ray films showed no instability in the lumbar vertebra; however, they did show slightly degenerative scoliosis. Magnetic resonance imaging (MRI) revealed no central spinal canal stenosis on T1- and T2-weighted images (Fig. 1). MRI demonstrated L5 spinal nerve compression in the L5/S1 extraforamen by a lateral type of disc herniation (Fig. 1). MRI provided clear images of the left sciatic nerve at the level of the buttocks (Fig. 1). The left side piriformis muscle was thicker than that on the right side (Fig. 1). To specify the origin of the painful site, we performed a nerve block at the two levels. One level was at the left L5 spinal nerve, and the other was the sciatic nerve at the level of the buttocks (Fig. 2). Both the left L5 spinal nerve block and the sciatic nerve block were effective. We diagnosed double nerve crush syndrome at two sites.
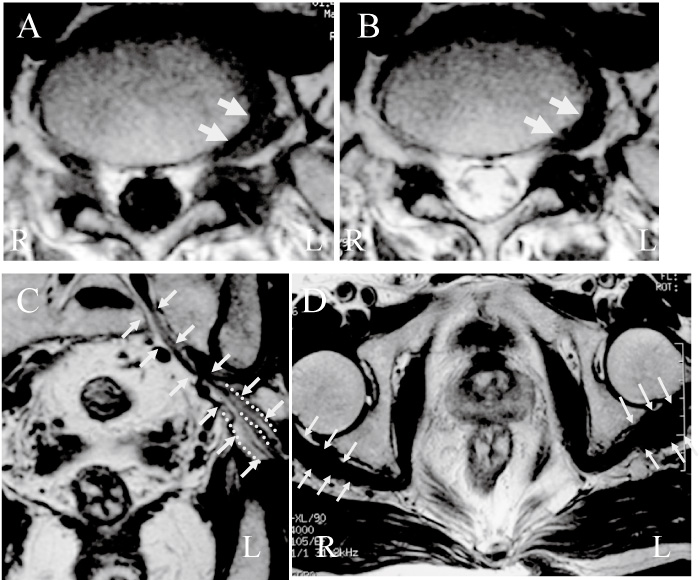
Fig. 1
Axial spin-echo T1- and T2-weighted magnetic resonance imaging (MRI) revealed left extraforaminal disc herniation at L5/S1 level before initial surgery (A and B; arrows). Frontal view of MRI revealed the left sciatic nerve (C; arrows), and axial view of MRI revealed piriformis muscle (D; arrows). Dotted lines indicated bifurcation of the sciatic nerve (C). The piriformis muscle on the left side was thicker than that on the right side R: right side, L: left side.
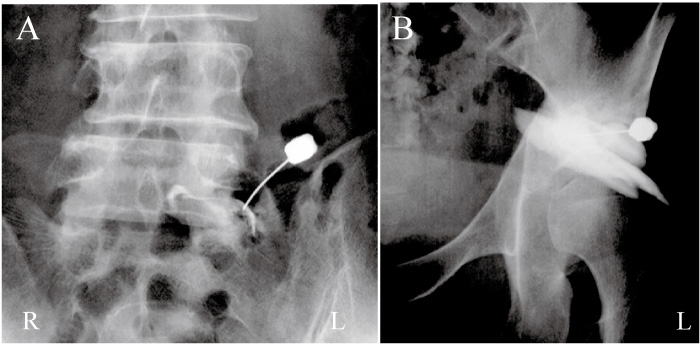
Fig. 2
Administration of lidocaine onto the left L5 spinal nerve (A) and the sciatic nerve at the level of the buttocks and (B) after injection of contrast medium was performed, and both blocks were effective.
Because conservative treatment was not effective, we planned second stage surgery. We performed an incision of the piriformis muscle for decompression of the sciatic nerve in October 2005. Intraoperative findings showed piriformis syndrome type B according to Beaton’s classification.[8]The sciatic nerve is divided into two branches and one main branch was compressed at the piriformis muscle. The extent of compression was more severe on external rotation of the hip joint than at the normal position. After incision of the piriformis, the sciatic nerve was decompressed. The pain decreased after surgery; however, it persisted for three months after the first surgery. We performed surgery to remove the herniated nucleus pulposus and for posterior lateral fusion with instrumentation in June 2006 (Fig. 3). Because we carefully found the L5 spinal nerve root running from the L4/5 level to the L5/S1 foramen level, we added L4/5 decompression and fusion. The L5 spinal nerve was severely compressed by disc herniation and the superior articular process of S1. The patient became symptom-free after surgery, and to date his postoperative course has been uneventful.
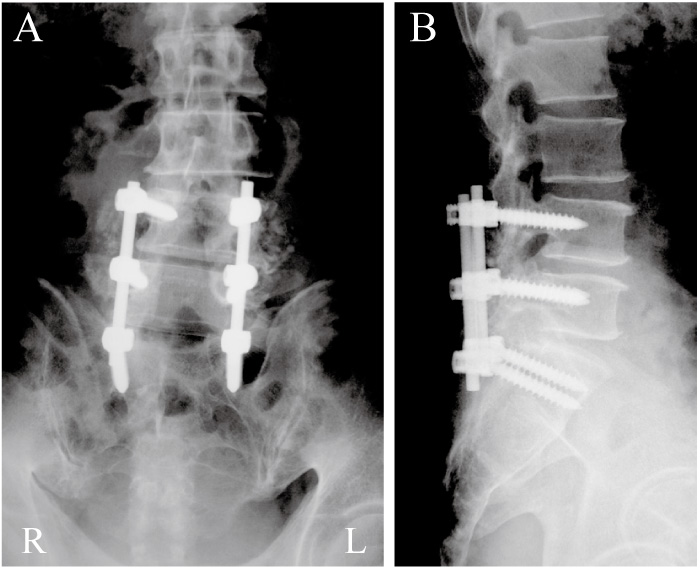
Fig. 3
Three months after incision of the piriformis muscle, removal of disc herniation and posterior lateral fusion with pedicle screws from L4 to S1 level was performed. A; antero-posterior view, B; profile view.
We searched the English-language medical literature and, to the best of our knowledge, no single case of sciatica caused by compression by a lumbar intervertebral disc and the piriformis muscle has been reported. Most common compression sites are the cervical spine, the cubital tunnel at the elbow joints, and the carpal tunnel at the wrist joints.
Piriformis syndrome only relatively rarely causes sciatic pain. Patients show severe sciatic pain at the site of the buttocks, and most cases occurred because of traumatic injury[9]. Tenderness in the buttock area, positive signs in Friberg’s and Pace’s tests, and sciatic nerve block are useful tools for the diagnosis of piriformis syndrome[10]. It is important to exclude spinal nerve compression at lumbar lesions, such as disc herniation and spinal canal stenosis. In the current case, we did not confirm traumatic injury in his past history; [10] however, MRI showed a thicker piriformis muscle compared with the intact side. There is a possibility that microtrauma thickened the piriformis muscle, and resulted in the nerve compression. He showed tenderness at his buttocks, a positive sign on Friberg’s and Pace’s tests, and relief of pain after sciatic nerve block. So, we confirmed a diagnosis of piriformis syndrome.
On the other hand, MRI showed extra-foraminal disc herniation at the L5/S1 level. The patient showed motor weakness of his left extensor hallucis longus and hypoalgesia in the lateral aspect of his lower legs corresponding to the L5 dermatome. L5 spinal nerve block was effective, and surgery for piriformis syndrome did not fully relieve his pain. Ultimately, surgery for his lumbar lesion diminished the pain, so we concluded that the pain originated partially from the lumbar lesion.
Double crush syndrome has been reported by several authors in cervical and peripheral nerve lesions.
In series of 1,000 cases of carpal tunnel syndrome (888 patients) there is a statistically significant incidence of bilaterality in patients with cervical arthritis. These findings lend further support to Upton’s double crush hypothesis[6]. Baba et al. examined 483 patients who underwent cervical decompression and peripheral nerve decompression surgery[11]. In these patients they confirmed 65 surgical cases (39 men and 26 women) with cervical myeloradiculopathy associated with entrapment neuropathy, the so called double crush syndrome. However, no author has been reported double crush syndrome at two sites such as the lumbar spine and the piriformis muscle.
The basic mechanism of double crush syndrome in animal models has been described by other authors[12,13]. Canine sciatic nerves to which compression was applied by using one or two clamps were studied. An incomplete conduction block and mild axonal degeneration were induced by a single compression. However, a complete conduction block and severe axonal degeneration could be induced by double compression. A good therapeutic effect was obtained by removing all the compression, but the effect was incomplete when either one of the compressions was retained[12]. Dellon et al. used a model of sciatic nerve minimal banding in the rat to investigate the effect on electrophysiological function of single or double band placement, concurrently or temporally separated[13]. This study confirmed that the existence of two sites of simultaneous compression will result in significantly poorer neural function than a single compression site. Sciatic nerves have been used in these experimental models, so we believe that we can extrapolate findings from these models to the present human situation.
In conclusion, we report double crush nerve syndrome by a lumbar disc herniation and from compression by the piriformis muscle. It is important to consider double crush syndrome in lumbar lesions and at the level of the buttocks.
腰椎椎間板ヘルニアと梨状筋症候群による2箇所で神経障害を起こした症例を経験したので報告する。患者は約6ヶ月間頑固な坐骨神経痛に苦しむ60歳男性であった。臨床所見として左臀部から下腿外側にかけての放散痛,バレーの圧痛点,フライバーグテストで(股関節屈曲・内旋)陽性を認めた。MRIではL5/S1の左外側型腰椎椎間板ヘルニアと左側の梨状筋部の肥厚が確認された。坐骨神経ブロック,左L5神経根ブロックを行い両者とも一時的な症状の軽減を認めたが,保存療法では疼痛コントロール不良であった。腰椎神経根レベルと梨状筋レベルでの2か所の部位での神経圧迫症状と考え,まず梨状筋解離術を行い坐骨神経の圧迫を解除したところ症状は軽減したが,術後3ヶ月痛みが残存した。そのため,外側型腰椎椎間板ヘルニアに対する神経根の除圧と後方固定を行い,術後症状は消失した。以上より,腰椎レベルと梨状筋レベル2箇所での神経圧迫障害を認めるダブルクラッシュ症候群の存在を念頭に入れることが必要である。
Department of Orthopedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
山口 毅,大鳥精司,山下正臣,古志貴和,山内かづ代,萬納寺誓人,鈴木宗貴,東 秀隆,金 民世,廣瀬 彰,高相晶士,青木保親,井上 玄,高橋和久: 腰椎椎間板ヘルニアと梨状筋症候群による2部位での神経障害の1例.
千葉大学大学院医学研究院整形外科学
Tel. 043-226-2117. Fax. 043-226-2116. E-mail: otokotakeshi@yahoo.co.jp
2009年9月8日受付,2009年9月30日受理.
