




Volume 86, Number 2
doi:10.20776/S03035476-86-2-P59
[Case Report]
Chiho Sato1), Shinya Yoshimoto1), Akikazu Udagawa1), Naoaki Rikihisa1) Yuichiro Kanazawa1), Yoshitaka Fukaya1), Shinsuke Akita1) Sara Shimizu2) and Kaneshige Sato1)
(Received November 6, 2009, Accepted November 25, 2009)
Giant secondary fistula in 20-year-old female patient involving the entire hard palate, measuring 32 × 40 mm, could be repaired with a tongue flap which is a simple procedure. The tongue flap used was large and thin without any lining except for turned-up flaps on its margin nor bony support.
At 6 years after surgery, slight contracture of the flap was evident, however, the surface of the flap was flat without any scar or wound, nor a fistula. The flap was fibrously hard and a weak touch sensation was evident at the margin of the flap. Narrowing of the tongue was evident extra-orally, however, deformity of the tongue was not remarkable intra-orally. Tongue movement, swallowing and taste were all normal.
Complex methods such as distant flaps or free flaps have been reported in such cases of big fistula over 3 cm in diameter, while the tongue flap has not been reported so far. However, in this case, the entire hard palate defect closure has been successfully completed by using tongue flap two-thirds in width of tongue combined with turned-up flap.
In the cases of the entire hard palate defects application of the tongue flap may be the procedure of choice before using complex methods.
complete hard palate defect, reconstruction, tongue flap, clinical results
Secondary palatal fistula is one of the most major complications after palatoplasty in cleft palate patients. Although small fistulas are closed with the use of local tissue, large fistulas are usually closed with a tongue flap [1-5]. However, in a large fistula which involves the majority of the hard palate, the application of the tongue flap for such a large fistula and its prognosis have been of interest.
The authors experienced a case of a post-palatoplasty giant palatal fistula which had formed a complete hard palate defect during the authors’ volunteer program in Nepal. This defect was closed with a tongue flap combined with local turned-up flaps. Tongue flaps are commonly used due to its durability against external forces [2-7]. However, in this case, the tongue flap was very large and did not constitute any lining except for turned-up flaps on its margin. Moreover, the majority of the hard palate bones were defective. Postoperatively, it was apprehensive whether the flap could withstand long term external forces. Fortunately, the authors had an opportunity to see this patient six years after operation.
The patient is a 20-year-old Nepali female with bilateral cleft lip and palate with no prior history of surgery. Although a push-back palatoplasty was performed simultaneously with bilateral cheiloplasty, postoperative necrosis resulted in the majority of the bilateral mucoperiosteal flaps. The follow-up examination of the patient at the following year revealed total bone deficit of the bilateral palatal shelves, resulting in a hard palate defect (Fig. 1)A tongue flap was planned for the closure of the defect 32 mm × 40 mm in size. Mucoperiosteal flaps of approximately 7 mm width were elevated and turned up from the margin of the fistula, followed by placement of a tongue flap of 33 mm width × 55 mm length × about 4 mm thickness over the mucoperiosteal flaps with 3-0 absorbable vertical mattress sutures ( Fig. 2, 3, 4)

Fig. 1
The preoperative findings of the palate. The bones of the both palatal shelves were almost all deficit and showed being hard palate defect of 32 mm × 40 mm in size.
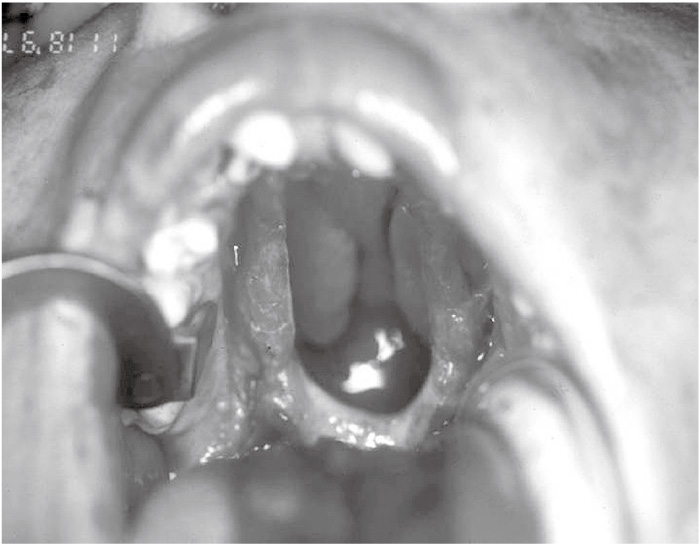
Fig. 2
The turning up mucoperiosteal flaps of about 7 mm width were elevated from the margin of the fistula.
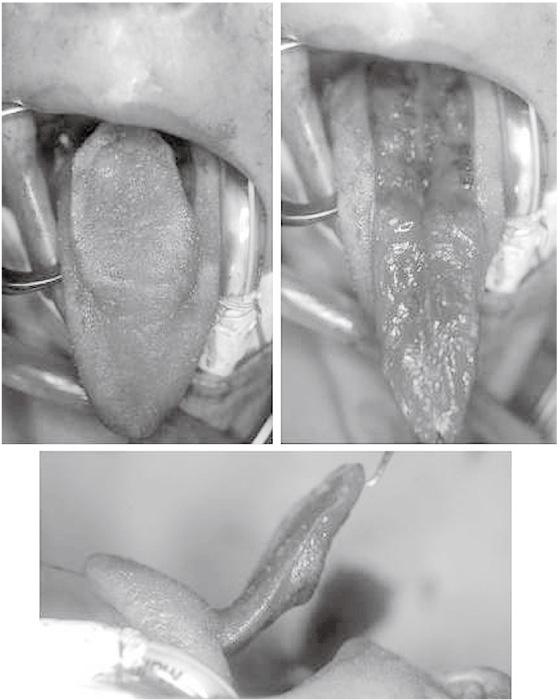
Fig. 3
A tongue flap of 33 mm width × 55 mm length × about 4 mm thickness was elevated. The flap contains just thin muscular layer.
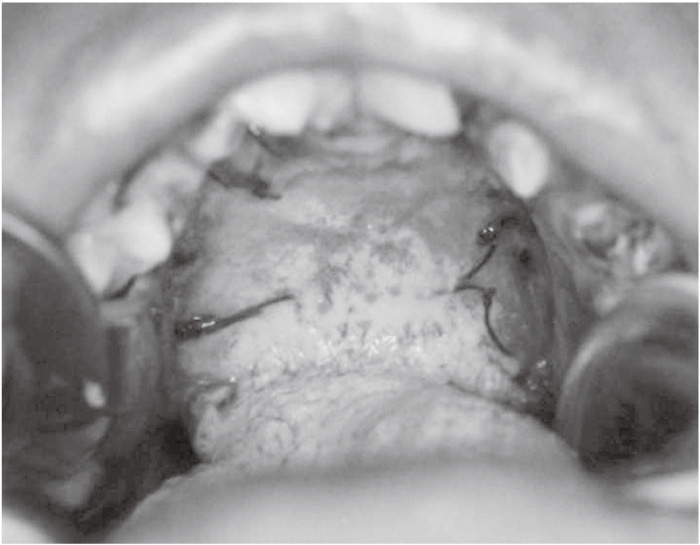
Fig. 4
The findings just before the flap separation: The tongue flap had been placed over the turning up flaps with vertical mattress sutures with 3-0 absorbable suture.
A thin muscular layer was contained in the flap. Raw surface of a few-millimeter-width around the flap, in addition to raw surface of 20 × 30 mm in size behind the flap was left untouched. Fixation of the tongue was not executed and the patient was placed on a semi-soft diet until flap separation. Postoperative course was uneventful and the flap was separated ten days after operation under general anesthesia. Although consultation of the patient was limited to a few days after flap separation, no complications were observed and the flap was observed to be intact (Fig. 5)
Unfortunately, consultation of the patient was not possible until 6 years later. At 6 years after surgery, slight contracture of the transferred tongue flap was evident, with a decrease in size to 30 × 35 mm. The surface of the tongue was flat without any scar or wound, nor a fistula (Fig. 6)
Although slight elasticity was evident on the center of the flap upon palpation, the flap was fibrously hard on the whole without any impression of either thinness or weakness. Although pain sensation was deficient, a weak touch sensation was evident at the margin of the flap. Narrowing of the tongue was evident extra-orally, however, deformity of the tongue was not remarkabl intra-orally (Fig. 7) The foliate papilla on the lateral edge of the tongue deviated to the dorsum of the tongue. Tongue movement, swallowing and taste were all normal. Although the palate was short, no evidence of food or liquid regurgitation was observed. The transferred tongue flap did not seem to have any effect on the patient’s daily life.
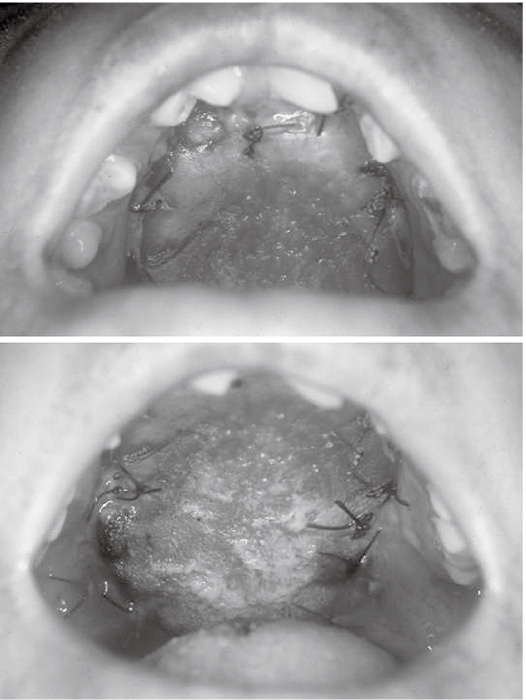
Fig. 5
The findings after the flap separation
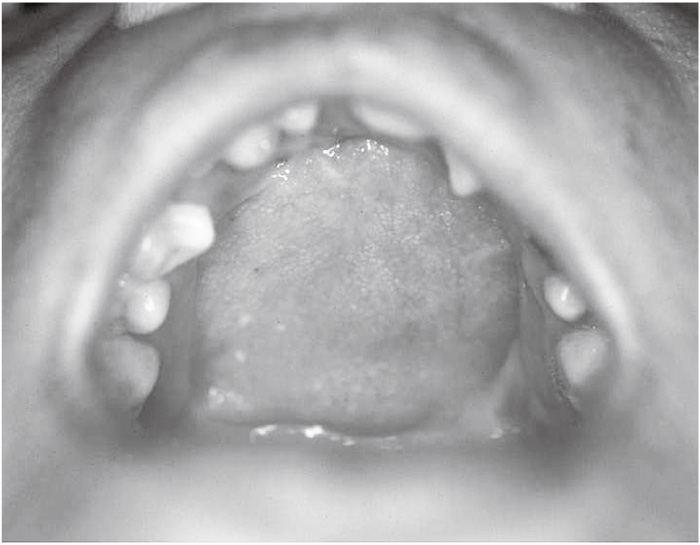
Fig. 6
The findings of the palate six years after the operation: The transferred tongue flap was 30 × 35 mm in size with slight contraction. The surface was flat without any scar or wound, nor a fistula.
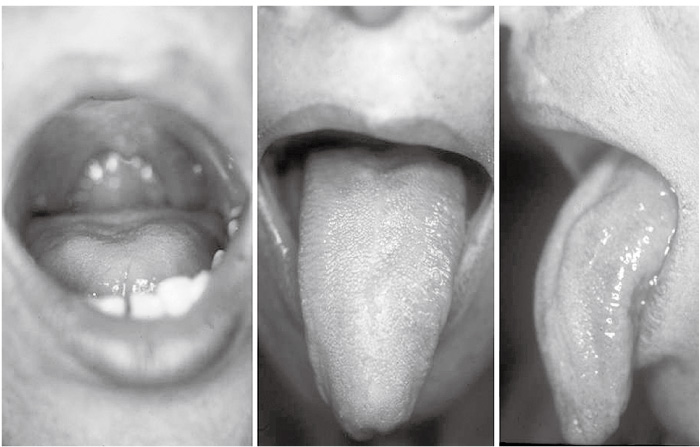
Fig. 7
The findings of the tongue 6 years after the operation: Narrowing of the tongue was evident extra-orally, however, deformity of the tongue was not remarkable intra-orally.
In cleft palate patients with fistulas which cannot be closed by local flaps, such as recurrent fistulas which had undergone previously unsuccessful attempts at closure, palatal fistulas with heavy scarring, and persistent large palatal defects, anteriorly-based tongue flaps are usually indicated; however, the use of cheek and nasolabial flaps, pedicled temporalis muscle flaps, various distant flaps and free flaps have also been reported [1,8,9] . To date, there have been no reports related to the closure of large fistulas with a tongue flap involving the majority of the hard palate as far as the authors have investigated. Although Posnick and Getz [1] suggest use of the temporalis muscle flap for fistulas larger than 3.0 cm, the tongue flap is an interesting alternative.
The tongue flap was first used by Lexer in 1909 [10] . Guerrero-Santos and Altamirano [2] initially reported the use of the tongue flap for closure of a large fistulae of the hard palate in a cleft palate patient in 1966, which was subsequently applied to numerous cleft palate patients by Jackson [3,4] . The tongue is approximately 72-73 mm in length, 45-49 mm in width and 21-22 mm in thickness [5] ; and two-thirds of its width, approximately 30 mm [5] , and 5 cm in length of the dorsum of the tongue can be elevated as a flap [3] . The flaps of this size have not been reported to cause tongue dysfunction. Some authors [6,7] have suggested raising the underlying muscle along with the tongue flap in order to provide durability and ensure vascularity. Posnick and Getz [1] suggested that this random-pattern musculo-mucosal flap should be about 1㎝ in thickness to include adequate muscle mass. Abe et al [5] used thin flaps of about 3 mm in thickness without muscle. In contrast to the bulky appearance of the musculo-mucosal flaps after inset, the thin flaps were reported to have lost this bulkiness, but have maintained its durability and its aesthetic appearance. Generally, mucoperiosteal flaps are elevated and turned up from the edges of the fistula as a lining of the flap, and the nasal side of the fistula is completely closed [1-4,8,9] . However, Abe et al [5] did not undergo this process of elevating and turning up the mucoperiosteal flap, instead simply deepithelialized a width of 2-3 mm around the fistula, and sutured the flap there with the lining of a free graft. The same method is also used by the authors; however, the use of a free graft for lining is not used.
In the present case, due to the largeness of the fistula diameter of 32 mm, the flaps were elevated and turned up from the edges of the fistula in order not to enlarge the tongue flap width any further, after which the tongue flap was on them. The tongue flap was approximately 33 mm in width, which was about two-thirds of the tongue width. In consideration of the large size of the fistula, the flap was elevated about 4 mm in thickness, which was slightly thicker than usual and contained a slight portion of the muscle layer in order to ensure durability and vascularity of the flap. The raw surface behind the flap remained untouched. Although this patient showed an entire defect of the bilateral palatal shelves, maturation of the scar around the fistula one year post-palatoplasty enabled elevation and turning up of local flaps, resultingly, the fistula was closed by placement of a flap two-thirds in width of the tongue over it. It is interesting to note that this large, thin tongue flap without complete lining and bone support could last without any problems. Thin tongue flaps have been found to show durability; however, in the present case, since the fistula was very large, with bone defects covering the majority of the bilateral palatal shelves, producing subsequent lack of bony support, the tongue flap used was thin without lining in a large portion of the flap center. At examination of the patient six years postoperatively, aside from a slight contraction of the flap, no wounds or scars were evident, and was aesthetically acceptable.
The authors suggest that even a complete hard plate defect may be closed with a tongue flap if local flaps are able to be elevated and turned up from the edges of the fistula, and more than two-thirds in width of the tongue can be elevated without producing dysfunction or disfiguration of the tongue shape.
Although it is rare to experience cases of complete hard palate defects after palatoplasty in advanced countries, they are not such a rarity in advancing countries. However, these defects may result in patients after tumor excision or post trauma. In such cases, application of the tongue flap may be the procedure of choice before using complex methods.
口蓋裂患者の口蓋形成術後に生じた硬口蓋全欠損に対して,舌弁と欠損部周辺のturned-upにて再建術を行った。欠損の大きさは縦40㎜,横32㎜で,舌弁の大きさは33×55×4㎜(厚さ)であった。使用した舌弁は大きく,薄く,ほとんどの部分が裏打ちをもたず,骨の支えも有しなかった。6年後の状態では,舌弁には軽度の収縮がみられたが,表面は平坦で,瘢痕や潰瘍,瘻孔など認めなかった。触診では線維性硬であり,舌弁の辺縁部に軽度であるが知覚が存在した。舌を口腔から突出させると舌はわずかに狭小であったが,気になる程度の変形ではなく,口腔内に収まっているときはほとんど変形はみられなかった。舌の運動や嚥下,味覚にも特に異常はみられなかった。
口蓋の全欠損という巨大な口蓋瘻孔を舌弁で再建したという報告はわれわれが渉猟し得た範囲内ではみられなかった。骨の支えもない舌弁による再建は長期結果が危惧されたが,術後6年の経過で特に異常は見られなかった。舌弁は,口蓋裂患者のみならず,腫瘍切除後の欠損などの再建にも有用と思われた。
佐藤知穂1),吉本信也1),宇田川晃一1),力久直昭1),金沢雄一郎1),深谷佳孝1),秋田新介1),清水サラ2),佐藤兼重1): 硬口蓋全欠損再建の1症例-舌弁による閉鎖と6年後の臨床結果.
1) 千葉大学医学部附属病院形成・美容外科,2) JFE川鉄病院形成外科
Tel & Fax. 043-226-2316. E-mail: keisei@office.chiba-u.jp
2009年11月6日受付,2009年11月25日受理.
