




Volume 86, Number 6
doi:10.20776/S03035476-86-6-P225
[Original Paper]
Takeshi Sainoh, Seiji Ohtori, Gen Inoue, Takana Koshi
Masaomi Yamashita, Kazuyo Yamauchi, Munetaka Suzuki, Sumihisa Orita
Yawara Eguchi, Nobuyasu Ochiai, Shunji Kishida, Kazuki Kuniyoshi
Junichi Nakamura, Yasuchika Aoki, Tetsuhiro Ishikawa, Masayuki Miyagi
Gen Arai, Hiroto Kamoda, Miyako Suzuki, Masashi Takaso
Tomoaki Toyone, Masashi Yamazaki and Kazuhisa Takahashi
(Received May 25, 2010, Accepted July 21, 2010)
Sacroiliac fixation using iliac screws for highly unstable lumbar spine with an improved fusion rate and clinical results have been reported. On the other hand, there is a possibility of clinical problems related to iliac fixation, including vertebral fracture at upper level and infection. So, the purpose of the current study was to investigate clinical results and complications after sacroiliac fixation using iliac screws.
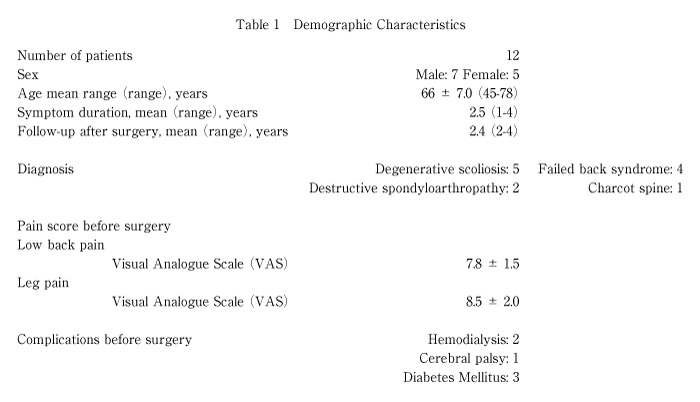
Twelve patients were evaluated. Diagnosis was degenerative scoliosis in 5 patients, failed back syndrome in 4 patients, destructive spondyloarthropathy in 2 patients, and Charcot spine in 1 patient. All patients underwent posterolateral fusion surgery using lumbar, S1 and iliac screws. We evaluated the pain scores, bone union, and complications by X-ray imaging and computed tomography during 2 years after surgery.
Pain scores significantly improved after surgery. All patients showed bone union at final follow up. Deep infection within 2 weeks after surgery was seen in 2 patients with diabetes mellitus. Compression fracture at upper level was seen in 2 patients 1 year after surgery.
Fusion rate and clinical results were excellent 2 years after surgery, however, rate of complications was high. We should take into consideration of complications to perform sacroiliac fixation using iliac screws for highly unstable lumbar spine.
Sacroiliac fixation, iliac screw, pain, surgery, complications
Posterior spinal instrumentation of the lumbosacral junction may be indicated in the surgical treatment of adult idiopathic scoliosis, intervertebral disc degeneration, and severe lumbosacral spondylolisthesis[1-3] . Despite advances in spinal implants and surgical techniques, pseudarthroses, hardware failure, and sagittal imbalance continue to be significant clinical problems. Some authors have reported that when S1 screws are used without augmentation, fusion rates are various (22%, 68%, 71%, and 89%), indicating technical difficulties with achieving lumbosacral fixation and fusion[4-7] . Proposed solutions have included intrasacral or trans-sacral rod fixation, buttress plates, sacral hooks, and various pedicle and iliac screw fixation techniques[8-11] .
On the other hand, there is a possibility of clinical problems related to compression fracture at upper level and infection after surgery. It is because of long fusion level and large surgical invasion to use iliac screws.
Therefore, the purpose of the current study was to evaluate the clinical results and complications during 2 years after sacroiliac fixation, using pain score, X-ray imaging, computed tomography (CT).
The ethics committee of our institution approved the protocol for the human procedures used in this study.
Twelve patients had low back and leg pain, continuing for at least 12 months. Patients were diagnosed on X-ray examination, myelography, CT after myelography, and magnetic resonance imaging (MRI). We excluded spinal tumor, infection, and trauma. All patients underwent decompression and posterolateral fusion surgery. Posterolateral fusion was performed using pedicle screws and a local and iliac bone graft. Lumbar, S1, and iliac screws were used in all patients. Anterior lumbar interbody fusion was added in 1 patient. Background details of the patients are shown in Table 1 (Table 1). Details of fusion level are shown in Table 2 (Table 2).
We evaluated low back, and leg pain before and after surgery. To evaluate the pain, the visual analogue scale (VAS) score (0, no pain; 10, worst pain) was recorded before and 2 years after surgery. Radiography was used for evaluation of bone union. Profile views of X-ray images at flexion and extension positions before and 3, 6, 12, and 24 months after surgery were evaluated. We defined bone union of less than 1.5° at one level as instability between the flexion and extension positions. CT was performed to evaluate bone union at 12 and 24 months after surgery. We defined bone union as bridging bone formation across the transverse process between adjacent vertebrae. Evaluation of bone union was blinded and performed by three observers. If at least two of the observers concurred, bone union was used to define the period of bone union.
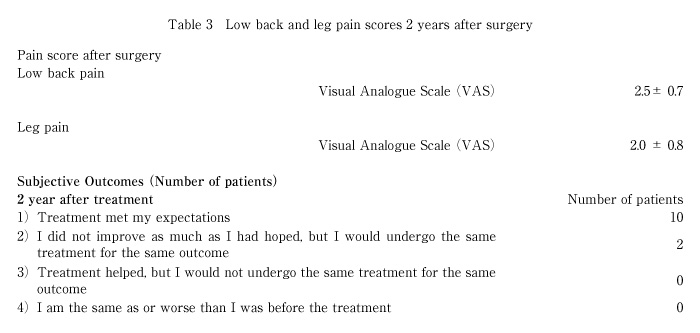
At 2 years after surgery, patients were asked to choose one of the following responses regarding their satisfaction with the surgical treatment according to criteria adopted by the North American Spine Society Low Back Outcome Instrument: (1) surgery met my expectations; (2) I did not improve as much as I had hoped, but I would undergo the same surgery for the same outcome; (3) surgery helped, but I would not undergo the same surgery for the same outcome; or (4) I am the same as or worse than I was before the surgery[12].
During 2 years, we evaluated complications such as vertebral fracture at upper level, superficial infection, and deep infection.
Data were compared using a Mann-Whitney U test. P<0.05 was considered statistically significant.
Table 1 (Table 1) shows demographic characteristics in patients before surgery. Diagnosis was degenerative scoliosis in 5 patients, failed back syndrome in 4 patients, destructive spondyloarthropathy in 2 patients, and Charcot spine in 1 patient. Complications before surgery were hemodialysis in 2 patients, cerebral palsy in 1 patient, and diabetes mellitus in 3 patients.
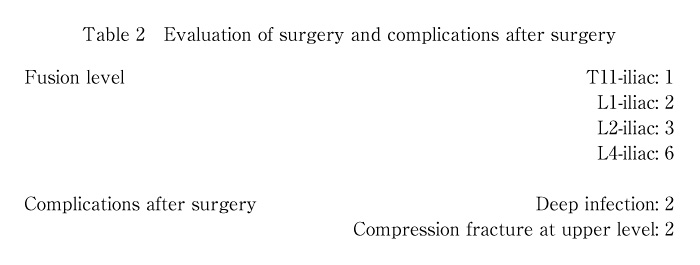
Intraoperative and postoperative measurements are shown in Table 2 (Table 2). Fusion level was most common from L4 to iliac in 6 patients. Longest fusion level was from T11 to iliac in 1 patient.
VAS score significantly improved after surgery compared with before surgery as shown in Tables 1 (Table 1) and 3 (Table 3) (P<0.01). Subjective outcome evaluated by patients was good in all 12 patients.
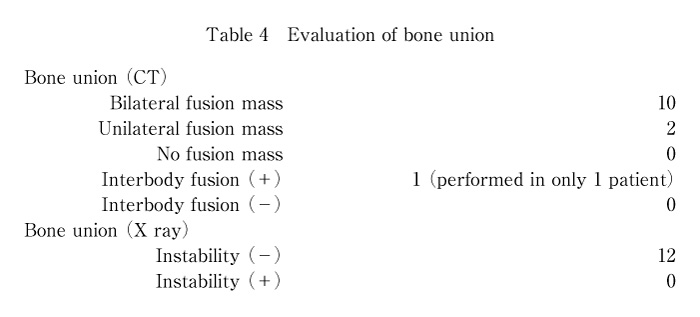
Evaluation of bone fusion is shown in Table 4 (Table 4). All patients showed bone union at final follow-up (2 years after surgery). The average period for bone union was 12 months (evaluation by X-ray imaging) and 12 months (CT) after surgery (Table 4) . Anterior interbody fusion was performed in 1 patient (failed back syndrome with cerebral palsy), and bone union was seen by X-ray imaging and CT 12 months after surgery.
Complications after surgery were seen in 4 patients. Deep infection within 2 weeks after surgery was seen in 2 patients with diabetes mellitus. Compression fracture at upper level was seen in 2 patients 1 year after surgery (Charcot spine; fusion level, T11-iliac and destructive spondyloarthropathy from hemodialysis; fusion level, L2-iliac) (Fig. 2).
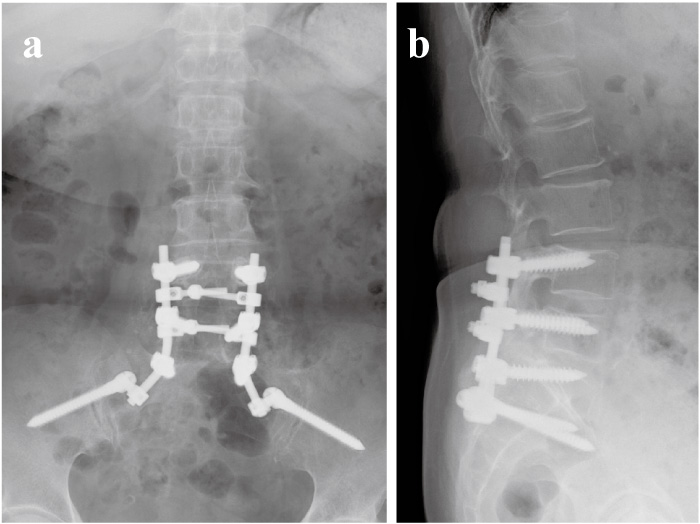
Fig. 1
The patient was a 67 year old woman with failed back syndrome. The patient underwent posterolateral fusion (L4 to iliac), and bone union was seen by X-ray imaging 12 months after surgery ((a) and (b)).
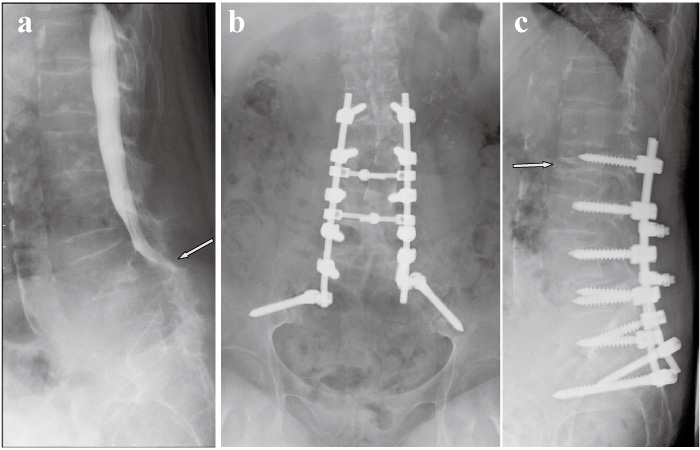
Fig. 2
The patient was a 65 year old woman with L4 destructive spondyloarthropathy from hemodialysis. Myelogram shows severe stenosis between L4 and L5 level (a). The patient underwent posterolateral fusion (L2 to iliac) (b and c). Compression fracture at L2 level was seen 1 year after surgery (c).
In the current study, we performed spinal fusion surgery using iliac screws for unstable lumbar deformity. Clinical results were good and spinal fusion was observed in all 12 patients. However, deep infection within 2 weeks after surgery was seen in 2 patients with diabetes mellitus. Compression fracture at upper level was seen in 2 patients 1 year after surgery.
We concluded that sacroiliac fixation using iliac screws provides stable fixation for unstable lumbar spine, however, rate of complication is high.
Kim et al. have analyzed the incidence of and risk factors for pseudarthrosis in long adult spinal instrumentation and fusion to S1[1]. The overall prevalence of pseudarthrosis following long adult spinal deformity instrumentation and fusion to S1 was 24%. Thoracolumbar kyphosis, older age at surgery (older than 55 years), and incomplete sacropelvic fixation significantly increased the risks of pseudarthrosis. Thus, S1 screws often fail with lumbosacral fusions, whereas L5-S1 pseudarthrosis is common in patients with deformity. Kuklo et al. have used iliac screws for high-grade spondylolisthesis, and report a follow-up of 2 years[3]. Bilateral iliac screws coupled with bilateral S1 screws provide excellent distal fixation for lumbosacral fusions with a high fusion rate (95.1%) in high-grade spondylolisthesis and long fusions to the sacrum. Tsuchiya et al. have investigated clinical and radiographical outcomes for lumbosacral fusion (in patients with spinal deformity) using a combination of bilateral sacral and iliac screws with a minimum 5-year follow-up[2]. Fusion rate was excellent (primary fusion rate 92.5%), and overall function and pain at ultimate follow-up was good, based on visual analog pain scales and Oswestry scores. These reports showed a high fusion rate using iliac screws for high-grade spinal deformity. In the current study, although problems in the patients included degenerative scoliosis, failed back syndrome, destructive spondyloarthropathy, and Charcot spine, fusion rate was 100%. Therefore we concluded that iliac screws were a useful tool for fixing unstable lumbar spine.
A systematic review of the English-language literature (published between January 1990 and June 2009) was undertaken to identify articles examining risk factors associated with and adjunct treatment measures for preventing surgical-site infections. For risk of infection with diabetes, seven case-control studies and 1 retrospective cohort study evaluated diabetes as a preoperative risk factor for postoperative surgical-site infection[13-17]. These studies reported a statistically significant association between diabetes and postoperative surgical-site infection[13-17]. The Japan Spine Research Society carried out a nationwide survey on the complications of spinal surgery, enrolling a total of 16,157 patients from 196 institutes, who had undergone spinal surgery during the 1-year survey period[18]. Of these, 1383 patients (8.6%) encountered postsurgical complications[18]. The incidence of complications associated with instrumentation surgery was 12.1%, which was twice as high as the incidence of complications associated with noninstrumentation surgery (6.8%). Infection rate was 0.9%. In the current study, deep infection within 2 weeks after surgery was seen in 2 patients with diabetic mellitus. Infection rate was 17%. Both case was revision surgery, and dead space was relative large for inserting the iliac screws. We concluded that diabetes mellitus and revision surgery are risk factors of infection to use iliac screw.
Compared with adolescent deformity, fusion for adult deformity is often associated with high rates of complications, including pseudarthorosis, instrumentation failure, junctional problem, and higher morbidity[19-20]. The major concerns in long fusions for adult lumbar deformity have focused on the distal fusion level and distal instrumentation failure[21,22], but there are few written reports concerning proximal adjacent segmental failure according to the level of proximal fusion in adult lumbar deformity. The radiographs and clinical records of 35 patients of adult lumbar deformity with more than 2-year follow-up after surgery were analyzed[23]. Compression fractures above the fusion and screw failure proximal to the end of the fusion were observed in 15 patients. Fusion up to throacolumbar junction (L2~T11) in surgical treatment of adult lumbar deformity had more proximal adjacent problems with poorer results. They concluded that fusion higher than T10 is recommended for adult lumbar deformity[24]. In the current study, compression fracture at upper level was seen in 2 patients 1 year after surgery (fusion level, T11-iliac and L2-iliac). Level of fusion was lower than T10 in both cases. We also recommend fusion higher than T10 in case of long fusion with iliac screws.
In conclusion, we evaluated fusion rate, clinical results, and complications 2 years after sacroiliac fixation. Fusion rate and clinical results were excellent 2 years after surgery, however, rate of complication was high. We should take into consideration of complication to perform sacroiliac fixation using iliac screws for highly unstable lumbar spine.
腸骨スクリューを使用した仙腸関節固定は不安定性の強い腰椎変形に対する手術成績を向上させると考えられている。しかしながら,強固な固定力をもたらす一方で,最上位の圧迫骨折,感染症等の問題も危惧される。従って本研究の目的は,腸骨スクリューを使用した仙腸関節固定後の臨床成績と合併症を検討する事である。 症例は12例であり,診断は変性側弯5例,腰椎再手術4例,透析による破壊性脊椎症2例,シャルコー脊椎1例であった。全ての患者は腰椎,仙椎,腸骨スクリューを用いた後側方固定術を行った。術前後の腰下肢痛,レントゲン,CTによる骨癒合,合併症を二年間に亘り調べた。腰下肢痛は術前に比較し有意に改善した。全ての患者で骨癒合が得られた。合併症として糖尿病を合併した患者2名に2週間以内の深部感染が認められた。また術後1年で最上位の圧迫骨折を2名の患者に認めた。 腸骨スクリューを使用した仙腸関節固定は術後2年成績では骨癒合,臨床成績共に良好であった。しかしながら合併症の危険性も高く,これらの使用に関しては充分にその危険性を考慮に入れて使用すべきである。
Department of Orthopedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
西能 健,大鳥精司,井上 玄,古志貴和,山下正臣,山内かづ代,鈴木宗貴,折田純久,江口 和,落合信靖,岸田俊二,国吉一樹,中村順一,青木保親,石川哲大,宮城正行,新井 玄,鴨田博人,鈴木 都,高相晶士,豊根知明,山崎正志,高橋和久: 腰椎脊椎変形に対する仙腸骨固定の成績と合併症.
千葉大学大学院医学研究院整形外科学
Tel. 043-226-2117. Fax. 043-226-2116. E-mail: sohtori@faculty.chiba-u.jp
2010年5月25日受付,2010年7月21日受理.
