




Volume 87, Number 1
doi:10.20776/S03035476-87-1-P7
[Case Report]
Shuichi Miyamoto, Seiji Ohtori, Gen Inoue, Takana Koshi
Masaomi Yamashita, Kazuyo Yamauchi, Munetaka Suzuki, Sumihisa Orita
Yawara Eguchi, Yasuchika Aoki, Tetsuhiro Ishikawa, Masayuki Miyagi
Gen Arai, Hiroto Kamoda, Miyako Suzuki, Masashi Takaso, Tomoaki Toyone
Yoshikazu Ikeda and Kazuhisa Takahashi
(Received July 21, 2010, Accepted August 11, 2010)
A 62-year-old patient presented with a 12-month history of severe sciatica. The patient showed tenderness of Valleix and lateral lower leg pain on his left side. MRI, myelogram, and radiculography revealed extraforaminal stenosis at the level of L5/S1. His symptoms disappeared after injection of lidocaine onto the L5 spinal nerve. The symptoms did not improve after conservative treatment, and surgery was performed under a diagnosis of neuropathy from far-out syndrome. For release of L5 spinal nerve compression, decompression and instrumented fusion surgery were performed. His symptoms disappeared immediately after surgery. Far-out syndrome itself is rare; however, it is important to consider this disease in cases of sciatica.
radiculopathy, far-out syndrome, pain, lumbar
Anatomically, the L5 spinal nerve can be compressed frequently by adjacent structures, osteophytes, or discs in the lateral and subarticular recesses of the spinal canal and intervertebral foramina[1-3]. In keeping with this concept of more lateral spinal nerve involvement, Wiltse et al. have pointed out that the L5 spinal nerve may, in fact, be compressed “far-out” by impingement of the transverse process of L5 against the ala of the sacrum in spondylolisthesis[4].
Some authors have reported that the L5 spinal nerve is compressed by a “far-out lesion”; however, reports are rarely found based on research of the English literature. Here we report a rare case of sciatica in a 62-year-old man, which is caused by compression of L5 spinal nerve by a “far-out lesion”
The protocol for human procedures used in this study was approved by our institution’s ethics committee. This report was also approved by the patient after informed consent. A 62-year-old man presented with a 12-month history of left sciatica involving the left lower extremities. He presented at our hospital in April 2008 with complaints of pain in his buttocks and the lateral aspects of his legs. There was apparent motor weakness of left extensor hallucis longus (manual muscle test: MMT 4/5). Sensory examination confirmed left hypoalgesia in the lateral aspect of his lower legs corresponding to the L5 dermatome. On the left side, a straight leg raising test was negative.
Plain X-ray films showed no instability in the lumbar vertebrae. Magnetic resonance imaging (MRI) revealed no central spinal canal stenosis on T1- and T2-weighted images (Fig. 1).
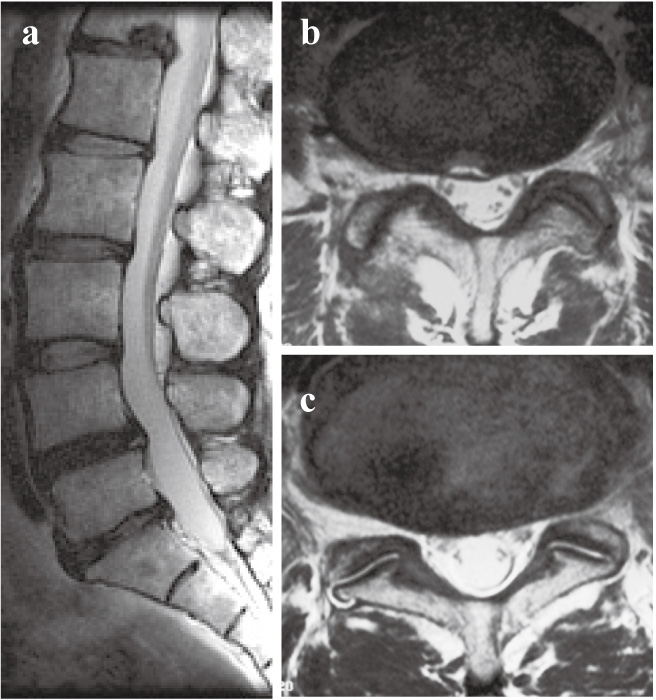
Fig. 1
Magnetic resonance imaging (MRI) revealed no central spinal canal stenosis on T2-weighted images (a, b (L4/5 level), and c (L5/S1 level)).
A myelogram and computed tomography (CT) following the myelogram showed slight stenosis and instability of the L4-L5 level (Fig. 2). Selective radiculography demonstrated that the L5 spinal nerve was compressed between the transverse process and the sacral alar (Fig. 3).
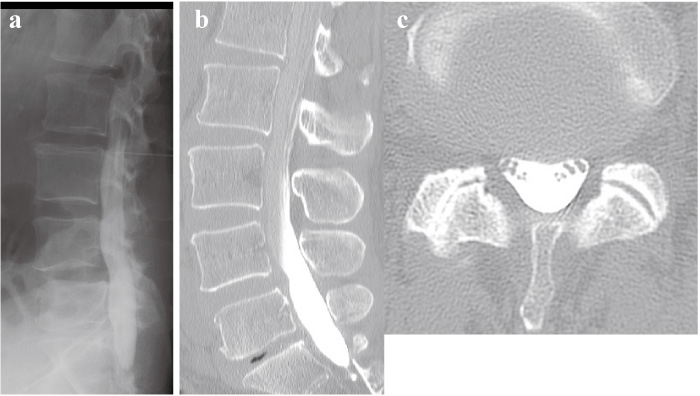
Fig. 2
A myelogram (a) and computed tomography (CT) following the myelogram (b and c) showed slight stenosis and instability of the L4-L5 levels.
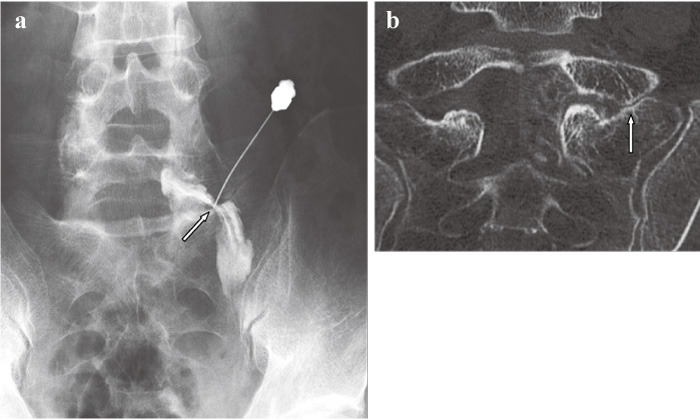
Fig. 3
Selective radiculography (a) and CT after selective radiculography (b) demonstrated that the L5 spinal nerve was compressed between the transverse process and the sacral alar (arrows).
To specify the origin of the painful site, we performed an L5 spinal nerve block using 1.5 ml of 1% lidocaine. The left L5 spinal nerve block was effective. We therefore diagnosed L5 spinal nerve compression between the L5 transverse process and the sacral alar.
Because conservative treatment was not effective, surgery was planned. We performed surgery to remove a part of the L5 transverse process and the S1 alar, and transforaminal lumbar interbody fusion with instrumentation in October 2008 (Fig. 4). Because on careful examination we found the L5 spinal nerve root running from the L4-L5 level to the L5-S1 foramen level, we added L4-L5 decompression and fusion. The L5 spinal nerve was not compressed in the spinal canal at the L4-L5 level; however, it was severely compressed by the L5 transverse process and the S1 alar. The patient became symptom-free after surgery, and to date his postoperative course has been uneventful. We performed selective radiculography 3 months after surgery. This radiculography demonstrated that the L5 spinal nerve was not compressed between the transverse process and the sacral alar (Fig. 5).
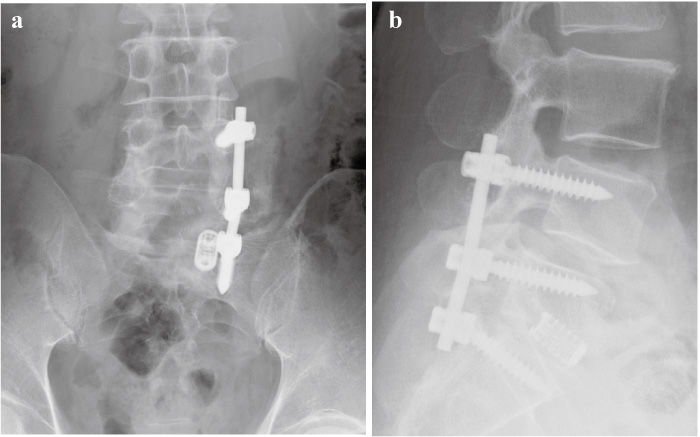
Fig. 4
We performed surgery to remove a part of the L5 transverse process and the S1 alar, and transforaminal lumbar interbody fusion with instrumentation.
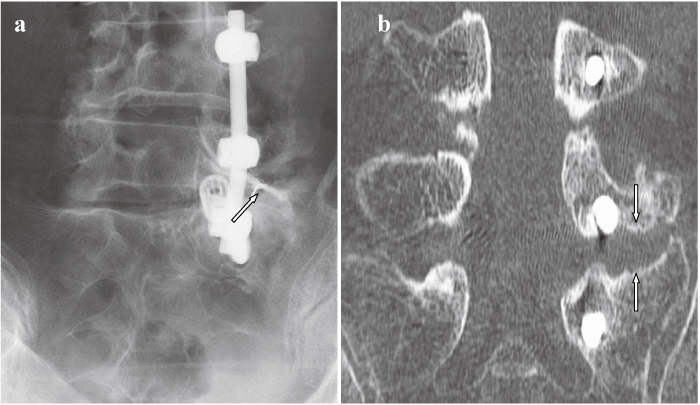
Fig. 5
Selective radiculography (a) and CT after selective radiculography (b) after surgery demonstrated that the L5 spinal nerve was not compressed between the transverse process and the sacral alar (arrows).
In the current study, we reported a rare case of sciatica in a 62-year-old man, which was caused by compression of the L5 spinal nerve between the L5 transverse process and the S1 alar. The patient became symptom-free after decompression of the L5 transverse process and the S1 alar.
Some authors have reported that the L5 spinal nerve is compressed between a part of the L5 transverse process and the S1 alar; however, reports are rarely found based on research of the English literature[5-9]. Some authors have reported that the L5 spinal nerve is compressed by several structures. Wiltse et al. have pointed out that the L5 spinal nerve may, in fact, be compressed “far-out” by impingement of the transverse process of L5 against the ala of the sacrum in spondylolisthesis[4]. Nathan et al. conducted a cadaveric study and found that the L5 vertebral body, the lumbosacral ligament, and the sacral ala formed a “lumbosacral tunnel,” and suggested the possibility of L5 spinal nerve compression in the “lumbosacral tunnel”[10,11]. On the other hand, several authors have reported that the L5 spinal nerve was compressed by a bony spur, and obtained pain relief after resection of the bone spur[5-7]. In the current study, the L5 spinal nerve was compressed between the L5 transverse process and the S1 alar without spondylolisthesis.
Generally speaking, diagnosis of far-out syndrome is difficult using plain X-ray film, CT, and MRI. Several authors have reported that selective nerve root infiltration and radiculography are useful for examining the condition of individual nerve roots[5-9]. They have the advantages of diagnosing the level of a lesion functionally by provoking or diminishing radicular symptoms as well as morphologically by depicting the running course of a spinal nerve. In the current study, selective radiculography demonstrated that the L5 spinal nerve was compressed between the L5 transverse process and the sacral alar. The left L5 spinal nerve block was effective for pain relief. Therefore, we concluded that the pain originated from the L5 spinal nerve compressed between the L5 transverse process and the sacral alar.
Several surgical methods have been reported to treat far-out syndrome, such as posterior resection of the L5 transverse process and the sacral ala, endoscopic posterior resection of the sacral ala, anterior resection of the L5 vertebral bony spur, and posterior decompression and instrumented surgery[5-9]. We selected posterior decompression and instrumented surgery between the L4 and S1 levels, because we were concerned about instability of the L5-S1 level after facetectomy. Furthermore, to find the L5 spinal nerve root running from the L4-L5 level to the L5-S1 foramen level, we added L4-L5 decompression and fusion.
In conclusion, we report a rare case of sciatica, which was caused by compression of the L5 spinal nerve between the L5 transverse process and the S1 alar. The patient became symptom-free after decompression of the L5 transverse process and the S1 alar. Radiculography clearly demonstrated a change in the L5 spinal nerve compression between the transverse process and the sacral alar after surgery.
Far-out syndromeよるL5神経根障害を生じた症例を経験したので報告する。患者は12ヶ月間強度な坐骨神経痛を呈する62歳男性であった。臨床所見として左臀部から下腿外側にかけての放散痛を認めた。MRI,脊髄造影検査,神経根造影にてL5/S1の外側部のfar-out syndromeが疑われ,左L5神経根ブロックを行い症状の軽減を認めた。しかしながら,保存療法では疼痛コントロール不良であった。Far-out syndromeによるL5脊髄神経圧迫症状と考え,除圧固定術を施行し,症状は消失した。以上より,far-out syndrome稀な疾患であるが,far-out syndromeでの神経圧迫障害を認める症例を念頭に入れることが必要である。
Department of Orthopaedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
宮本周一,大鳥精司,井上 玄,古志貴和,山下正臣,山内かづ代,鈴木宗貴,折田純久,江口 和,青木保親,石川哲大,宮城正行,新井 玄,鴨田博人,鈴木 都,高相晶士,豊根知明,池田義和,高橋和久: Far-out syndromeによりL5神経根症を呈した1例.
千葉大学大学院医学研究院整形外科学
Tel. 043-226-2117. Fax. 043-226-2116. E-mail: sohtori@faculty.chiba-u.jp
2010年7月21日受付,2010年8月11日受理.
