




Volume 87, Number 4
doi:10.20776/S03035476-87-4-P159
[Original Paper]
Ichiro Shimoyama1), Akio Yoshida1,2), Takako Yugeta2), Katsunao Saeki1,3)
Fumiaki Hayashi1), Hidekiyo Yoshizaki1) and Ryohei Shimizu1,4)
(Received February 18, 2011, Accepted April 1, 2011)
Quantitative analysis was tried for cognitive functions for 115 volunteers, aged 21 to 88 years. Reaction time (RT) was used for visual (V-RT), auditory (A-RT), vibratory cues (V-RT), right-left-orientation cognition (RL-RT), and short-term-memory cognition (STM-RT) for the same subjects. Subjects were asked to judge a cue presented whether the right or left side and push a button at the same side as the cue presented, as for V-RT, A-RT, and V-RT. Subjects were asked to read sentences as “Push the right/left button, or Push the same button as the previous instruction” and RTs were measured for the former sentence as for RL-RT, and the latter sentences for STM-RT. RTs were analyzed with the exponential regression, and all RTs increased with increasing age significantly. Mean RT and standard deviation was 0.48±0.17sec for V-RT, 0.44±0.28sec for A-RT, 0.51±0.20sec for V-RT, 9.12±4.01sec for RL-RT, and 5.26±2.45sec for STM-RT. The analysis of variance showed significant among RTs (P<0.0001). The exponential regression analysis showed [V-RT]=0.222×e(0.011×[AGE]), R2=0.274; [A-RT]=0.090×e(0.022×[AGE]), R2=0.339; [V-RT]=0.227×e(0.011×[AGE]), R2=0.251; [RL-RT]=3.129×e(0.014×[AGE]), R2=0.129; and [STM-RT]=1.863×e(0.014×[age]), R2=0.132. The RTs increased with aging, so were good to differentiate dementing diseases from natural aging for further study.
cognition, aging, reaction time, quantitative analysis
CT; computed tomography, MRI; magnetic resonance imaging
Neurofibrillary tangles, microscopic cerebral infarction, and neocortical Lewy bodies all noted for the aged and those neuropathology correlated something to dementia, and the clinical evaluation for cognitive function showed declining with increasing age[1] . Morphological examination with CT or MRI scanning is good to detect a neoplasm, cerebral vascular diseases or cerebral atrophy, but cognitive function could not be estimated only with those examinations. Little age-related decline was evident in the absence of these lesions[1] . Dissociation sometime occurs between cerebral morphology and cognitive function[1] , dementing patients sometime show normal findings on CT or MRI scanning and they show deteriorated scores on the Mini-Mental States[2] or other memory tests, and vice versa. Cognitive function is important to differentiate dementia from natural aging. Nerve conduction is deteriorating with increasing age[3,4] , and auditory evoked potentials show also deteriorated with increasing age[5,6] . Higher brain function is sensitive to aging[7,REFF] , and memory and/or cognition are main symptoms of dementia, but the cognitive function is difficult to examine qualitatively. Questionnaire or interview tests prepare us non-parametric ranked scores subjectively. Objective parametric studies are poor for the cognitive functions. And objective parametric tests would be helpful to examine early dementing disorders, and important to differentiate them from natural aging. Cognitive functions were studied in an objective parametric way with the reaction time (RT) for visual, auditory, vibratory, right-left-orientation and short-term-memory functions. The reaction times were studied for natural aging.
Reaction time was studied with 2 push buttons and a personal computer (cf. Chiba Medical Journal 2005; 81: 103-6.). The visual stimuli were displayed on a TV-monitor 40 cm apart in front of a subject, a white circle (0.95 degrees visual angle for central visual field and 1.9 degrees for peripheral visual field) with a black background was displayed in a central (1.5 degrees) or peripheral visual field (16 degrees) at random, right or left at random, and upper or lower at random. And the subject was asked to push the button as quick as he/she could at the same side as the visual cue displayed on the monitor, and 32 reaction times were measured and the mean reaction time was used for discussion (visual-RT).
Auditory stimuli were used as a click sound of 0.1 msec from a headphone at 25, 40 or 60 dB (SPL) at random, for the right or left ear randomly. The subject was asked to push the button as quick as he/she could at the same side as the stimulus. Six stimuli were done for each side, and the mean RT was used for discussion (auditory-RT).
Vibratory stimuli were used with 2 discs (8cm diameter) at 83 Hz, the subject was asked his/her palms to put on the discs at the same side and asked to push the button as quick as he/she could at vibratory sensation. Four stimuli were done for each side at random, and mean reaction time was used for discussion (vibratory-RT).
Reaction times were measured on recognizing the sentence “Push the right button/ Push the left button” displayed on the TV-monitor. The subject was asked to react on the instruction as quick as possible to hit the button, and RT was measured four times for each side randomly (right-left-RT).
Reaction times were measured for the short term memory, i.e., the subject was asked to hit the button on recognizing the sentence “Put the button at the same side as the previous instruction” just after a short distraction task for a minute (memory-RT).
One hundred and fifteen volunteers participated in this study after obtaining informed consent. They had no history of visual, auditory, sensory and neurological disorders and they were 73 three males and 42 females aged from 21 to 88 years (mean 63.8, standard deviation 14.2 years).
The data were discussed with the exponential regression analysis.
Figure 1-A(Fig. 1) showed the visual-RT and the age. Reaction times increased on increasing age. The regression analysis showed RTs increased with increasing age; [RT]=0.222×e(0.011×[AGE]), R2: 0.274 (correlation coefficient: 0.52). The mean RT was 0.48 sec (standard deviation: 0.17).
Figure 1-B(Fig. 1) showed the auditory-RT and the age. Reaction times increased on aging. The regression analysis showed RTs increased with increasing age; [RT]=0.090×e(0.022×[AGE]), R2: 0.339 (correlation coefficient: 0.58). The mean RT was 0.44 sec (standard deviation: 0.28).
Figure 1-C(Fig. 1) showed the vibratory-RT and the age. Reaction times increased on aging. The regression analysis showed RTs increased with increasing age; [RT]=0.227×e(0.011×[AGE]), R2: 0.251 (correlation coefficient: 0.50). The mean RT was 0.51 sec (standard deviation: 0.20).
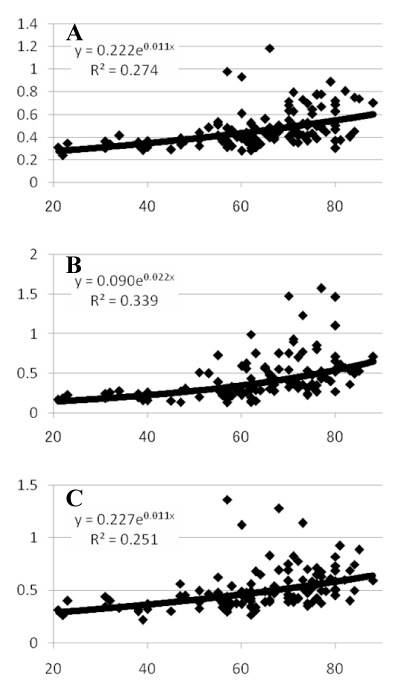
Fig. 1
A: The upper graph was visual cognition-reaction time and age. A regression line showed[Reaction Time]=0.222×e(0.011×[AGE]), R2: 0.274, mean RT was 0.48 sec±0.17 (standard deviation). B: The middle graph was auditory cognition-reaction time and age. A regression line showed[Reaction Time]=0.09×e(0.022×[AGE]), R2: 0.339, mean RT was 0.44 sec±0.28 (standard deviation). C: The lower graph was vibratory cognition-reaction time and age. A regression line showed[Reaction Time]=0.227×e(0.011×[AGE]), R2: 0.251, mean RT was 0.51 sec±0.20 (standard deviation). The abscissa represents reaction time in sec, and the ordinate represents age in years, for all graphs.
Figure 2-A(Fig. 2) showed right-left-RT and age. Reaction times increased on aging. The regression analysis showed RTs increased with increasing age; [RT]=3.129×e(0.014×[AGE]), R2: 0.129 (correlation coefficient: 0.50). The mean RT was 9.12 sec (standard deviation: 4.01).
Figure 2-B(Fig. 2) showed memory-RT and age. Reaction times increased on aging. The regression analysis showed RTs increased with increasing age; [RT]=1.863×e(0.014×[age]), R2: 0.132 (correlation coefficient: 0.36). The mean RT was 5.26 sec (standard deviation: 2.45).
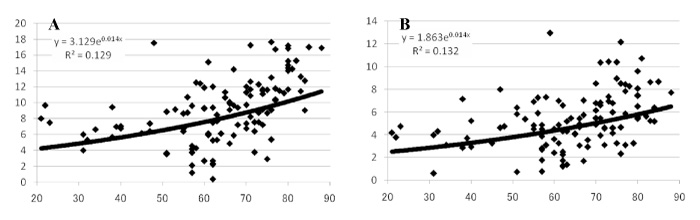
Fig. 2
A: The upper graph was right-left-orientation-cognition-reaction time and age. A regression line showed[Reaction Time]=3.129×e(0.014×[AGE]), R2: 0.129, mean RT was 9.12 sec±4.01 (standard deviation). B: The lower graph was short-term-memory-cognition-reaction time and age. A regression line showed[Reaction Time]=1.863×e(0.014×[AGE]), R2: 0.132, mean RT was 5.26 sec±2.45 (standard deviation). The abscissa represents reaction time in sec, and the ordinate represents age in years, for all graphs.
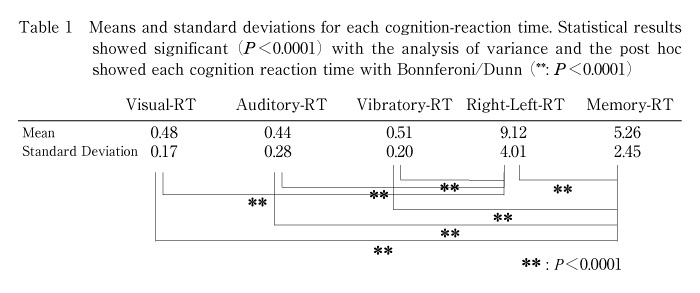
Table-1 (Table 1) showed mean RTs and standard deviations for the cognitive functions. The analysis of variance showed a significant difference among the cognitive functions (P<0.0001), RT for right-left-orientation showed the longest among them and RT for short-term-memory showed the next long time. The post hoc test showed significant differences between right-left-RT and RTs for other functions (P<0.0001), and between memory-RT and RTs for other functions (P<0.0001).
The cognitive RTs were all increased significantly with increasing age for visual-, auditory-, vibratory-, right-left-orientation-, and short-term-memory-cognition.
Reaction times showed no differences among visual and auditory and vibratory cognition. But, right-left-RT, memory-RT needed longer time to react the cues, because these latter 2 RTs needed much time to read and understand the sentences, and the former 3 RTs needed only to recognize the cues presented to the subject. The length of the sentence was longer for memory-RT than right-left-RT, but right-left-RT took longer time than memory-RT. The task for right-left-RT was to understand the sentence and decide the side, which needed longer time than the task for memory-RT. The task for memory-RT also needed to understand the sentence and recall the recent memory of the side. The RTs might represent the difficulty for the processing. The output in RTs was to push a button and the time needed from the primary motor cortex to muscles should be constant among the cognition tasks. The input in the RT was to look at the monitor for visual-, right-left-, and memory-RTs, and the time for the visual signals to get to the primary visual cortex should be constant, and the processing time might be sensitive to the difficulty in cognitions. The speed of face cognition had been reported to depend on the age[9], which was consistent with our results.
Memory disturbance is one of main symptom for dementing patients[7], which was consistent with our results.
Reaction time might be contaminated with arbitrary factors, but subjects were asked to react as quick as they could on recognizing cues, and if they did so and the statistical analysis would minimize the contamination. The RTs can examine the aged to differentiate dementing diseases from natural aging.
This work was supported by Development stage, City Area Type, Regional Innovation Cluster (1001047001001), Program Project for Developing Innovation Systems (1001047) funded by MEXT, Japan.
神経の加齢はCT/MRIスキャンでは皮質萎縮/脳室拡大とか無症候性梗塞などで観察され,はたらきにはミニメンタルステツとか改訂長谷川式簡易知能スケールなどの質問票が必須となる。脳梗塞などの局所所見がなくても,大脳高次機能とりわけ認知症核症状の記憶・認知機能にも加齢はおこる。CT/MRIスキャンで異常所見が無いのに認知症例もあり,その逆にも遭遇する。形態と機能は必ずしも並行しない。認知機能は質問表とか積木などの行動を点数化して用いるのがほとんどで,客観的方法としては機能的MRI・脳磁図・単一光子放射断層撮影・陽電子放射断層撮影で検査できるが軽症では行われない。認知機能を客観的定量的に解析するために反応時間(RT)をもちいて,視覚・聴覚・振動覚・左右認識・短期記憶認識におけるそれぞれの認知RTについて計測し,加齢変化について検討した。対象者は21~88歳の平均63.8歳,標準偏差14.2歳の男73女42名の115名から同意を得て記録した。被検者に視力障害・聴力障害・感覚障害・脳卒中などの既往歴はない。平均RTは,視覚認知RT: 0.48±0.17秒,聴覚認知RT: 0.44±0.28秒,振動覚認知RT: 0.51±0.20秒,左右認識認知RT: 9.12±4.01秒,短期記憶認知RT: 5.26±2.45秒であった。すべてのRTと年齢との相関は有意であった。分散分析では,左右認識認知RTと他のRT,短期記憶認知RTと他のRTと有意差が認められた。RTが年齢と有意に相関して長くなるという今回の結果から,将来的な研究によって,RTで認知症と健康者を鑑別できる可能性が示唆された。
1) Frontier Medical Engineering, Chiba University, Chiba 263-8522.
2) Yoshida Hospital, Mobara 299-4113.
3) Department of Neurosurgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
4) Shimizu Neurosurgical Hospital, Ichihara 290-0062.
下山一郎1),吉田明夫1,2),弓削田多賀子2),佐伯直勝1,3),林 文明1),吉崎英清1),清水良平4): 認知機能の加齢変化-定量的解析-.
1) 千葉大学フロンティアメディカル工学研究開発センター
2) 吉田医院
3) 千葉大学医学研究院脳神経外科
4) 清水脳神経外科
Tel. 043-290-3118. Fax. 043-290-3118. E-mail: ichiro@faculty.chiba-u.jp
2011年2月18日受付,2011年4月1日受理.
