




Volume 87, Number 5
doi:10.20776/S03035476-87-5-P181
[Original Paper]
Shigeru Sugaya1), Tamami Kasetani2), Zhong Qiu-Ji1)
Wen Zhi Guo1), Akikazu Udagawa3), Jun Nomura4)
Katsuo Sugita4), Reiko Ohta5) and Nobuo Suzuki1)
(Received February 25, 2010, Accepted April 14, 2011)
Shinrin-yoku, forest-air bathing and walking, is expected to be beneficial for the health of humans, but its effectiveness has not been clarified unequivocally by biophysical and biochemical analysis. In the present study, the amounts of oxidative damages after forest walking were compared with those after walking in an urban environment. Twelve female patients with rheumatoid arthritis (RA) aged 48-62 years-old and eleven healthy female volunteers aged 48-52 years-old walked in Chiba City at noon for 1 hr, and then moved by bus to a forest park on the first experimental day, followed by staying for one night in the park area. On the next day, they walked in the forest at noon for 1 hr according to their physical ability. RA patients in one group after forest walking showed decreased amounts of serum hydroperoxide and increased urine 7,8-dihydro-8-oxodeoxyguanosine (8-OHdG) levels, as estimated by a Diacron-Reactive Oxygen Metabolites (dROM) assay and an ELISA method, respectively, in comparison with those after city walking. In RA patients, the amounts of salivary IgA (sIgA), as estimated by an ELISA method, increased after forest walking. The amounts of serum matrix metalloproteinase-3 (MMP-3), as estimated by an ELISA method, decreased after forest walking.
These results were concordant with the notion for the suppression of oxidative stress and modulation of immunological and/or enzymatic physiological functions by forest walking.
shinrin-yoku (forest-air bathing and walking), rheumatoid arthritis, oxidative stress, salivary IgA, matrix metalloproteinase-3
Recreation and relaxation in a forest environment is called “shinrin-yoku” (forest-air bathing and walking) in Japan. Following shinrin-yoku, favorable effects were reported on human physiological functions[1-3]. Moreover, volatile compounds, which are produced and secreted from forest plants, were reported to have biological effects and suggested to cause changes in physiological functions after shinrin-yoku; for instance, decreased blood pressure and salivary cortisol concentration, and increased saliva secretion[3].
However, there are no reports on favorable effects of shinrin-yoku in diseases whose conditions may be related to reactive oxygen stress. Reactive oxygen species have been implicated in the pathogenesis of rheumatoid arthritis (RA), although the pathophysiological basis of RA is not yet fully understood[4]. RA is a chronic progressive autoimmune disorder characterized by symmetric erosive synovitis and sometimes shows involvement of multi-system disturbance in the human body[5]. The long-term outcome of this disease is characterized by significant morbidity, loss of functional capacity, and increased mortality[6,7]. In RA patients, antioxidant capacity levels of the plasma were suggested to be lower than those in healthy persons[5]. The production levels of reactive oxygen species in patients with RA has been found to be more than five-fold greater than either healthy control subjects or patients with nonrheumatic diseases[8], and the amounts of plasma lipid peroxidation products were significantly higher in patients with RA than those in healthy subjects[5]. In RA patients, the amounts of urinary 8-OHdG, recognized as a biomarker of oxidative DNA damage by endogenously generated oxygen radicals[9], were higher than those in healthy donors[10].
Recently, a novel automated, and rapid method for the measurement of reactive oxygen metabolites has been reported; the d-ROM assay is convenient, reliable, reproducible and cost effective, and gives results within a short time for the estimation of serum hydroperoxide levels[11]. Hydroperoxides are one of the dehydrogenation and peroxidation products of several cellular components including proteins, peptides, amino acids, lipids, and fatty acids. In the present study, the amounts of serum hydroperoxide and urine 8-OHdG, as markers of oxidative status, were estimated in RA patients and healthy volunteers who experienced shinrin-yoku. We also measured the amounts of sIgA and serum MMP-3 proteins. sIgA serves as a main immunological defense of mucosal surfaces in saliva[12], and moderate exercise results in an increased sIgA level[13]. MMP-3 is thought to be involved in the pathogenesis of RA, since the synovial fluid from RA patients contains a large amount of MMP-3; therefore, the serum concentration of MMP-3 is a useful marker for predicting bone damage in the early stage of RA[14]. The data obtained from volunteers after forest walking were compared with those after city walking to determine whether shinrin-yoku was beneficial for RA patients.
The Ethics Committee of Chiba University approved the study protocol, and written informed consent was obtained from all volunteers. Twenty three women (48-62 years-old) who volunteered, and gave informed consent, participated in the study. The volunteers were 2 groups; a rheumatoid arthritis patients group (RA) consisting of 12 women, aged 48 to 62 years, and a healthy group (HG) consisting of 11 women, aged 48 to 52 years.
Experiments were performed in September and October. Both experiments were conducted in an urban environment around Chiba City railway station (Chiba Prefecture, Japan) and in a forest environment at Nippon Aerobics Center (Chiba Prefecture, Japan), 20 km from the station. The volunteers stayed at a hotel in Chiba City and took a walk for 90 min in the city from 10:00 am. Volunteers were instructed to refrain from eating or drinking (except for water) after 9:00 am to minimize possible food debris and stimulation of salivation. After walking in the city, saliva, urine, and blood were obtained from the volunteers. Saliva samples were collected using an absorbent cotton roll. Urine samples were obtained from each individual and stored at -80℃ until analysis. Venous blood was obtained in vacutainers without additives, allowed to clot for 30 min at room temperature, and centrifuged (3,000 x g for 20 min) for serum collection. After the samples were obtained, the RA patients, healthy volunteers, doctors, nurses, and other staff moved by bus to the hotel in Nippon Aerobics Center. Volunteers stayed at the hotel, and on the following day took a walk for 90 min in the forest. After walking, the volunteers again supplied saliva, urine, and blood samples. The air temperature and humidity were measured by digital thermo-hygrometer (CHINO HN-K, Saitama, Japan). The atmospheric pressure was analyzed using an Eco Edge Nature and Weather Predictor (Speedtech Ins., Great Falls, VA, USA). The meteorological data for each session of shinrin-yoku are summarized in Table 1 (Table 1).
The oxidative status was evaluated by measuring hydroperoxide concentration in the serum according to an automated method using a kit (d-ROM test, Diacron, Grosseto, Italy); hydroperoxides are products of dehydrogenation and peroxidation of several cellular compounds including proteins, peptides, amino acids, lipids and fatty acids. When the samples are dissolved in an acidic buffer, the hydroperoxides are converted to alkoxy and peroxy radicals. The radicals oxidize an additive (N,N-diethyl-paraphenylendiamine) to the corresponding radical cation, and the concentration of the persistent species was determined spectrophotometrically (absorption at 505 nm)[15]. The serum amounts of hydroperoxides were indicated as U. CARR (Carratelli Units), where 1U. CARR corresponds to 0.8 mg/l H2O2.
Urine samples were centrifuged at 13,000 x g for 10 min, and the supernatant was used after appropriate dilution. Estimation of the 8-OHdG concentration was performed using a competitive ELISA kit (Japan Institute for the Control of Aging, Shizuoka, Japan). The estimation range was 0.64-2,000 ng/ml. Creatinine concentration was also estimated using a Pure-AutoS CRE-L kit (Daiichi-kagaku, Tokyo, Japan). Data are calculated as amount of 8-OHdG (ug/ml) per creatinine (g/ml) and showed as the relative ratio.
Volunteers were instructed to chew a cotton roll for about 2-3 minutes, which was then placed inside a centrifuge tube, and saliva was obtained by centrifugation. A Salimetrics HS-IgA kit (Salimetrics LLC, State College, PA) was used for the quantitative measurement of sIgA levels. Data are calculated as amount of sIgA (ug) per saliva volume (ml) and showed as the relative ratio.
The concentration of MMP-3 protein in sera was estimated by a one step sandwich ELISA system using a human MMP-3 kit (Panaclear MMP-3; Daiichi Pure Chemicals Co, Tokyo, Japan). Data are calculated as amount of MMP-3 (ng) per serum volume (ml) and showed as the relative ratio.
Results were expressed as the relative mean and standard deviation (SD). The statistical analyses were done using Student’s t test with Excel 2003 software (Microsoft, Tokyo, Japan). A P value of less than 0.05 denoted the presence of a statistically significant difference.
Although RA is recognized as autoimmune disorders, it is believed that weather influences rheumatic pain[16]. Therefore meteorological data were collected (Table 1). Each level of serum hydroperoxide estimated after forest walking was compared with that after urban walking in individual volunteers. In all 5 volunteers with RA in September, the post-forest walking levels were lower than the post-urban walking levels (Fig. 1A(Fig. 1), P=0.008). In addition, total RA volunteers combined for September and October, showed tendency for lower hydroperoxide levels after forest walking than after urban walking (Fig. 1C(Fig. 1), P=0.095). All 6 HG volunteers in the October group showed lower hydroperoxide levels after forest walking than after urban walking (Fig. 1B(Fig. 1), P=0.004).
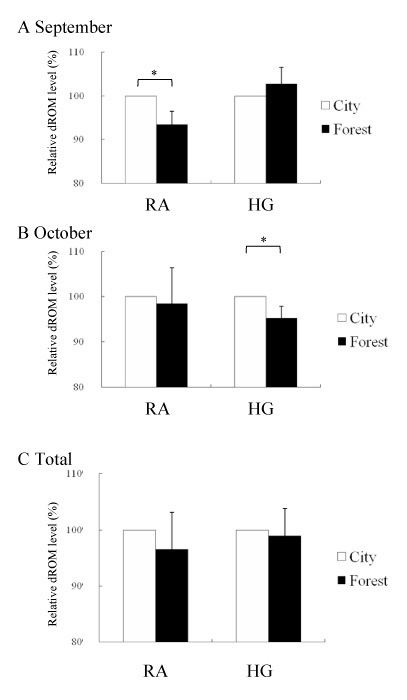
Fig. 1
Comparison of hydroperoxide concentrations in serum samples between post-urban and post-forest walking in RA patients and HG volunteers. Experiments were performed in September (A) and in October (B). Total data of each group are shown in column (C). (A) RA patients (N=5), HG volunteers (N=5). (B) RA patients (N=7), HG volunteers (N=6). White and black bars indicate relative d-ROM levels in serum samples after urban and forest walking, respectively.
Oxidative conditions were also compared using the levels of urinary 8-OHdG (estimated as the 8-OHdG/creatinine ratio) between post-urban and post-forest walking. In all 5 volunteers with RA in September, their 8-OHdG levels after forest walking were higher than those after urban walking (Fig. 2A(Fig. 2), P=0.038). In the total RA group, they showed tendency for higher levels of 8-OHdG after forest walking than after urban walking (Fig. 2C(Fig. 2), P=0.063). In addition, HG volunteers in October showed tendency for higher 8-OHdG levels after forest walking than after urban walking (Fig. 2B(Fig. 2), P=0.090).
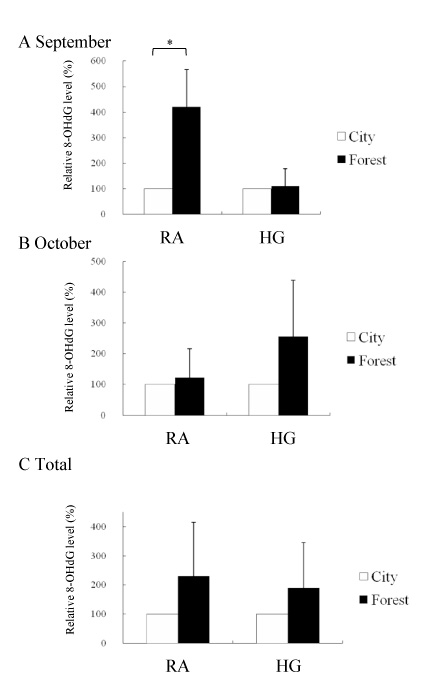
Fig. 2
Comparison of urinary 8-OHdG concentrations between post-urban and post-forest walking in RA patients and HG volunteers. Experiments were performed in September (A) and in October (B). Total data of each group are shown in column (C). (A) RA patients (N=5), HG volunteers (N=5). (B) RA patients (N=7), HG volunteers (N=6). White and black bars indicate relative 8-OHdG levels in urine after urban and forest walking, respectively.
The levels of sIgA and MMP-3 were examined comparatively between post-urban and post-forest walking. In the total RA group, the participants showed higher levels of sIgA after forest walking than after urban walking (Fig. 3C(Fig. 3), P=0.001). For the total HG volunteers, they showed higher levels of sIgA after forest walking than after urban walking (Fig. 3C(Fig. 3), P=0.043). In September, both RA (P=0.011) and HG volunteers (P=0.045) showed lower MMP-3 levels after forest walking than after urban walking (Fig. 4A(Fig. 4)). Furthermore, in total RA patients the MMP-3 levels after forest walking were lower than those after urban walking (Fig. 4C(Fig. 4), P=0.002).
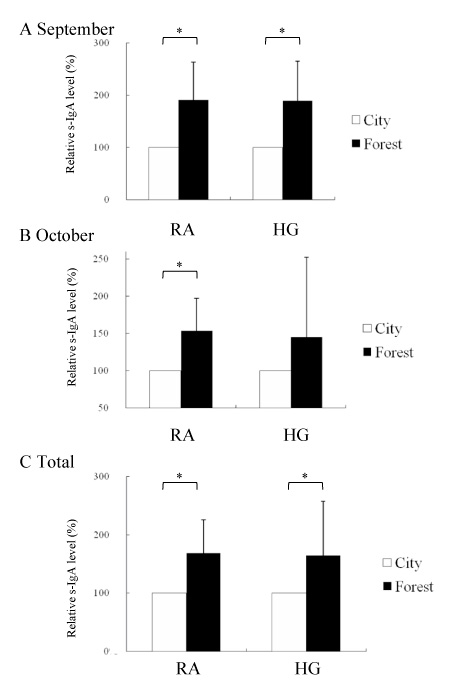
Fig. 3
Comparison of salivary IgA concentrations between post-urban and post-forest walking in RA patients and HG volunteers. Experiments were performed in September (A) and in October (B). Total data of each group are shown in column (C). (A) RA patients (N=5), HG volunteers (N=5). (B) RA patients (N=7), HG volunteers (N=6). White and black bars indicate relative sIgA levels in saliva after urban and forest walking, respectively.
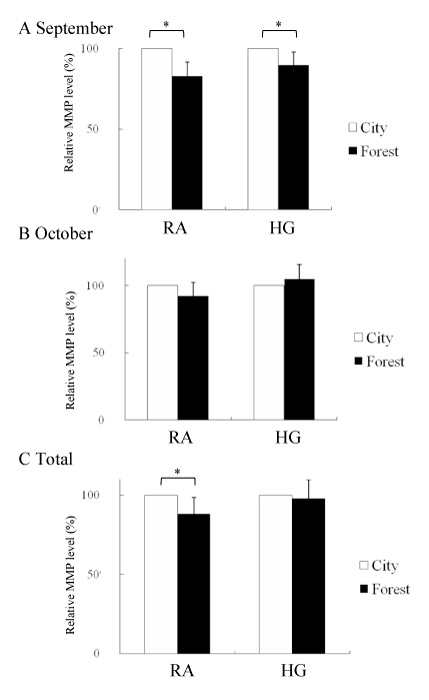
Fig. 4
Comparison of MMP-3 concentrations in serum between post-urban and post-forest walking in RA patients and HG volunteers. Experiments were performed in September (A) and in October (B). Total data of each group are shown in column (C). (A) RA patients (N=5), HG volunteers (N=5). (B) RA patients (N=7), HG volunteers (N=6). White and black bars indicate relative MMP-3 levels in serum after urban and forest walking, respectively.
Exercise therapy is expected to be essential and fundamental for the treatment of patients with RA, and walking in a forest environment was evaluated in this study for biochemical markers with beneficial effects for RA patients; improved levels of serum hydroperoxide, urinary 8-OHdG, sIgA and MMP-3 in RA patients and HG volunteers. The physiological status of each volunteer was analyzed comparatively between urban and forest environments. It is difficult to measure the physiological effects of short time stay, therefore in this research volunteers were staying the hotel in forest area and next day the data after forest walking were collected. The potential for reactive oxygen species production in RA patients has been suggested to be greater than that of healthy control subjects and patients with non-rheumatic diseases[8]. The average hydroperoxide levels in the RA group after urban walking was 368.8 +/- 31.2, which was higher than those of the HG group, 292.4 +/- 28.3. Our results demonstrated that the levels of serum hydroperoxide were higher in RA patients than in healthy volunteers.
In all volunteers in the RA group in September, the hydroperoxide levels after forest walking were significantly lower than those after urban walking, but such a decrease was observed in only 3 of 7 volunteers in October (Fig. 1A and B). There was a difference in the humidity between the urban and forest environments: 7.2% in September and 34.4% in October, and the temperature: 3.2 ℃ in September and 6.1 ℃ in October (Table 1). Interestingly, a close relationship was suggested between RA symptoms and relative humidity[17]. Thus, a comparison of the environmental parameters of the experimental conditions between September and October indicated that the temperature and humidity might influence the effectiveness of the suppression of oxidative stress in RA. The weather conditions may be an important factor when the effectiveness of exercise therapy is considered for RA patients.
In addition to hydroperoxide, the urinary excretion of 8-OHdG reflects the oxidative condition, such as the integrated rate of oxidative DNA damage and the repair of DNA[18]. After shinrin-yoku, higher levels of urinary 8-OHdG were observed in the RA group in September (Fig. 2A). Thus, in September enhanced excretion of 8-OHdG was observed in RA patients after shinrin-yoku in accordance with lowered levels of serum hydroperoxide. Environmental conditions including shinrin-yoku might affect the oxidative stress conditions including serum hydroperoxide and urinary 8-OHdG in RA patients.
In HG volunteers, probable accordance of the above two oxidative damage products was seen in October (Figs. 1B and 2B) Thus, further studies on the effectiveness of shinrin-yoku will be also necessary on oxidative stress conditions in healthy persons.
Decreases in immunological potentials under stress conditions were reported previously[19]. Here, the volunteers showed higher levels of sIgA after forest walking (Fig. 3C),. Thus the activity of immunological defense components may be modulated after forest walking. Recently, Yamaguchi et al.[3]reported that salivary amylase activity, which is considered as a stress-induced marker, was reduced in a forest environment compared with an urban environment. As saliva sampling is non-invasive and stress-free, the measurement of sIgA and amylase levels and/or activities will be a good marker of the physiological effects caused by a forest environment on not only RA patients but also in healthy persons.
The serum concentration of MMP-3 is usually a marker in the early stage of RA, and the suppression of MMP-3 production may be an effective therapeutic approach for patients with early RA[14]. MMP-3 levels were decreased in the RA group after forest walking (Fig. 4 and C). Previous reports have shown that forest environments have excellent physiological effects on patients with allergies or respiratory diseases[20,21]. Together with these reports the present results suggested that staying and walking in a forest atmosphere might be introduced for rehabilitation programs for RA patients as an exercise therapy in the future.
We thank the staff of Chiba Rehabilitation Center for technical support. This work was supported in part by a Grant-in-Aid from the following organizations: Chiba Prefecture Welfare Foundation, the Smoking Research Foundation, the Tokyu Foundation for a Better Environment, the Tsuchiya Foundation, the Kieikai Research Foundation, and a Grant-in-Aid from the Ministry of Education, Science and Culture of Japan.
「目的」森林浴はヒトの健康によいとされるが,その効能を生理・生化学的解析により明らかにした研究はほとんどない。本研究では,森林散策後の体内の酸化傷害物量のレベルを測定し,都市散策後のレベルと比較した。
リウマチ患者女性12名(48-62歳)および健常人女性11名(48-52歳)について,千葉市内で昼間90分間の散策を行った。その日のうちにバスで移動し,森林環境で宿泊後,翌日,森林環境で昼間1時間の散策を各人の生理活動能力に従い行った。
都市散策後と森林散策後を比較した結果,森林散策後の血清においては,1群のリウマチ患者でDiacron-Reactive Oxygen Metabolites (dROM)法により測定したヒドロペルオキシド量は減少し,尿中では,ELISA法により測定した8-OHdG量は増大した。また,リウマチ患者の唾液中では,ELISA法により測定したIgA量は,森林散策後に高くなった。ELISA法により測定したMMP-3量は森林散策後の方が都市散策後に比べ,低い値を示した。
以上より,森林浴は,体内での酸化ストレス度を抑制することが示唆された。また,免疫力ないし生理酵素機能の調節が示唆された。
1) Department of Environmental Biochemistry, Graduate School of Medicine, Chiba University, Chiba 260-8670.
2) Chiba Prefectural Agriculture And Forestry Research Center, Sammu 289-1223.
3) Department of Plastic and Aesthetic Surgery, Chiba University Hospital, Chiba 260-8677.
4) Department of Clinical Medicine, Faculty of Education, Chiba University, Chiba 263-8522.
5) Chiba Rehabilitation Center, Chiba 266-0005.
菅谷 茂1),綛谷珠美2),紀 仲秋1),郭 文智1),宇田川晃一3),野村 純4),杉田克生4),大田令子5),鈴木信夫1): 森林浴を体験したリウマチ患者の血清ヒドロペルオキシド,MMP-3,尿中8-OHdG,唾液イムノグロブリンA量に関する調査.
1) 千葉大学大学院医学研究院環境影響生化学
2) 千葉県森林研究センター
3) 千葉大学医学部附属病院形成外科
4) 千葉大学教育学部養護教育学
5) 千葉リハビリテーションセンター
Tel. 043-226-2041. Fax. 043-226-2041. E-mail: s-sugaya@faculty.chiba-u.jp
2010年2月25日受付,2011年4月14日受理.
