




Volume 87, Number 6
doi:10.20776/S03035476-87-6-P245
〔Case Report〕
Miyako Suzuki, Seiji Ohtori, Gen Inoue, Sumihisa Orita, Yawara Eguchi
Yasuchika Aoki, Tetsuhiro Ishikawa, Masayuki Miyagi, Gen Arai, Hiroto Kamoda
Yoshihiro Sakuma, Yasuhiro Oikawa, Go Kubota, Masashi Takaso, Tomoaki Toyone
Akimitu Kuroiwa, Toru Ishizaka1), Goro Matsumiya1) and Kazuhisa Takahashi
(Received July 11, 2011, Accepted August 18, 2011)
We present a case report of a 72-year-old male patient with a solitary metastasis, probably from a renal carcinoma, to the lumbar vertebra at the L3 level, which we treated surgically with total en bloc spondylectomy (TES). At the time of admission, the patient had motor weakness in his right lower extremity due to compression of spinal nerve roots. We planned TES with spinal instrumentation by a combined posterior and lateral approach. His symptoms improved after surgery, and he eventually could walk by himself. We did not select a direct anterior approach because we were concerned about possible adhesions that might have developed following a prior anterior resection of a renal tumor. However, we were forced to leave in place the anterior portion of the L3 vertebra because the lateral approach prevented us from accessing the segmental artery on the contralateral side. Based on this experience, we would normally recommend a combined posterior and anterior approach for TES of a lumbar lesion in cases without any special circumstances.
total en bloc spondylectomy, lumbar, limitation, tumor
The spine is the most frequent site of bone metastases, and the incidence of spinal metastases is increasing[1]. The most common tumors metastasizing to the spine are breast, lung, renal, prostate, thyroid, melanoma, myeloma, lymphoma and colorectal cancer[2]. Older techniques of decompression without stabilization yielded poor outcomes, but results from a 2005 multicenter study indicated that modern surgery (including combined anterior and posterolateral approaches with stabilization) plus radiotherapy was associated with a better outcome than radiotherapy alone and that quality of life often improved after surgery[3]. A second multicenter randomized study published the same year, by Patchell et al., also found benefit from adding surgery to radiotherapy, specifically that adding aggressive surgical decompression and instrumented stabilization to radiotherapy halved the mortality rate compared with radiotherapy alone[4]. More recently, total en bloc spondylectomy (TES) has gained acceptance as the treatment of choice for resecting spinal tumors entirety[5,6]. However, TES at lower lumbar spine levels is technically challenging because of the local anatomy, including the presence of major vessels (e.g. aorta and the vena cava). We present here a case report involving the use of TES to treat a renal tumor in the L3 vertebra, and based on our experience, we discuss the limitations of a posterior-lateral surgical approach.
The protocol for human procedures used in this study was approved by our institution’s ethics committee. Our patient reviewed and approved this report.
A 72-year-old man was diagnosed with a spinal tumor and referred to our hospital with a four-month history of lower back pain. Sixteen years earlier, at age 56, he had undergone right nephrectomy for a clear cell renal carcinoma. At the time of admission to our hospital, his lower back pain had become severe, and he had developed right sciatica in conjunction with right leg motor weakness, leaving him unable to stand or walk. Other complaints at this time included frequent urination and constipation.
Physical examination demonstrated motor weakness of the right iliopsoas (Manual Muscle Test: MMT 3/5), quadriceps (Manual Muscle Test: MMT 3/5), biceps femoris (Manual Muscle Test: MMT 3/5), tibialis anterior (Manual Muscle Test: MMT 3/5) and extensor hallucis longus (Manual Muscle Test: MMT 4/5). Sensory examination confirmed hypoalgesia of the right L3 distribution area. Laboratory investigation of C - reactive protein (CRP) level, erythrocyte sedimentation rate (ESR) and enzyme assays indicated that his liver and renal function were within normal limits.
No abnormal findings were found on x-rays. Magnetic resonance imaging (MRI) showed that the tumor had invaded into most of the L3 vertebral body and to a lesser extent into the L3 lamina, spinous process, and the right L3 pedicle. The tumor also had invaded into the spinal canal at the L3 level, severely compressing the neural elements at the same level (Fig. 1).
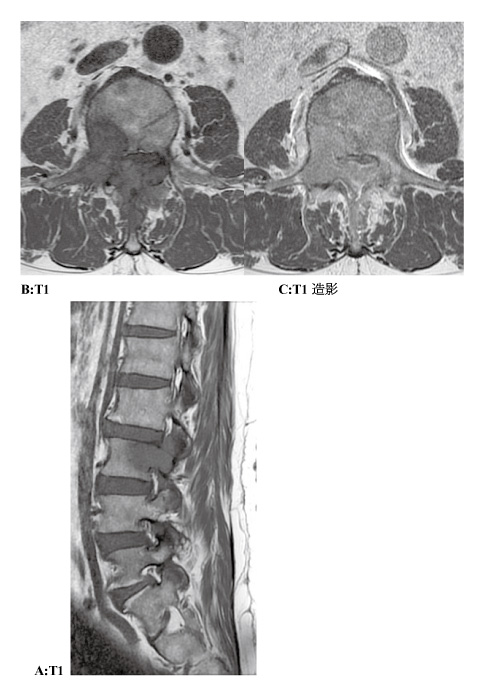
Fig. 1
Preoperative magnetic resonance imaging (MRI) of the lumbar spine. A: Midline sagittal image of the lumbar spine. The tumor expanded into the epidural space of L3. The tumor of the L3 posterior arch expanded into the paravertebral muscle. B: T1 of axial image at the L3 level. The tumor invaded the vertebral body, right pedicle, right transverse process, and spinous process of the L3 vertebra. C: gadolinium-enhanced of axial image at the L3 level. The tumor was enhanced by gadolinium.
Computed tomography (CT) showed that the lumbar lesion was osteolytic (Fig. 2).
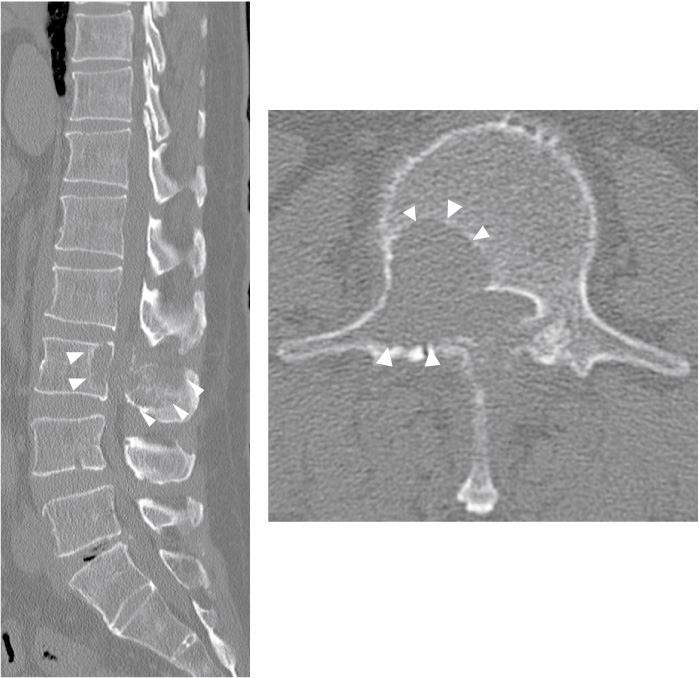
Fig. 2
Preoperative computed tomography (CT) scan at the L3 level. The vertebral body, right pedicle, right transverse process, and spinous process of the L3 vertebra were affected and osteolytic (The arrows).
Systemic CT (e.g., brain, neck, chest, and abdomen) did not detect any tumor foci other than the lumbar lesion. Bone scintigraphy did not show any other bony metastases. Angiography showed dilation of the L3 segmental arteries and an extremely hypervascular tumor (Fig. 3).
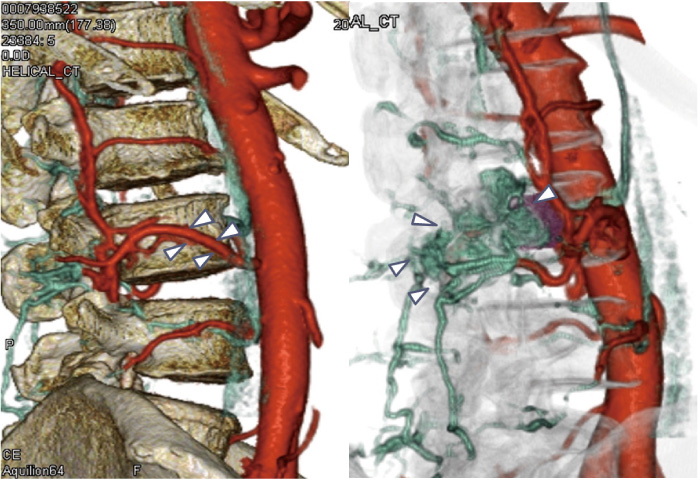
Fig. 3
Preoperative angiography showed that the L3 segmental arteries had dilatation and the tumor was extremely hypervascular (arrows).
The patient’s Tokuhashi score (12 points) and Tomita score (3 points) indicated a prognosis of more than six months survival[7-9], based upon which we decided to treat his tumor with total en bloc spondylectomy (TES), a treatment approach that includes aggressive spinal tumor resection and spinal reconstruction. We planned a TES with spinal instrumentation via a posterior-lateral approach, avoiding a directly anterior approach because of the possibility of adhesions from his prior renal tumor resection.
One day before the operation, we embolized the main feeder arteries of the L3 segmental arteries and their branches. The operation itself was in two steps: (1) posterior total en bloc spondylectomy and spinal reconstruction; (2) anterior ligation of the segmental vessels, anterior dissection around the vertebral body and the tumor, and anterior fusion.
We placed the patient in a prone position on the Hall frame and made a posterior midline incision.
We exposed the posterior elements of T11-S1, inserted pedicle screws into the bilateral pedicles of T11-S1 (except for L3), and connected a rod to the bilateral pedicle screws.
On the right side of the tumor dominance, the L3 lamina and pedicles had tumor involvement. Epidural tumor extension at the L3 level severely compressed the dural tube. We carefully removed both sides of the L3 vertebral arch, pedicle, and transverse process, followed by decompression. Considerable bleeding occurred, mainly from the tumor itself and the venous plexus in the spinal canal, which was stopped by surgical cotton tamponade. We then washed the surgical site with saline, inserted a drain, and sutured the wound (Fig. 4).

Fig. 4
Operative view of the last stage of the posterior approach.
With the patient in a supine position, we undertook an extraperitoneal lateral approach. The descending aorta and the inferior vena cava were dissected, and the left segmental artery and vein were ligated at the L3 level and cut near their junction with the aorta or the vena cava. We had vascular surgeons perform this procedure because of the technical complexities arising from the dilation of the segmental artery. We then dissected around the vertebral body and the portion of the tumor external to the vertebral body, maintaining tumor margins. After detaching the L2/3 and L3/4 discs, we removed most of the L3 vertebral body, inserted a mesh cage, and fixed it in place (Fig. 5).
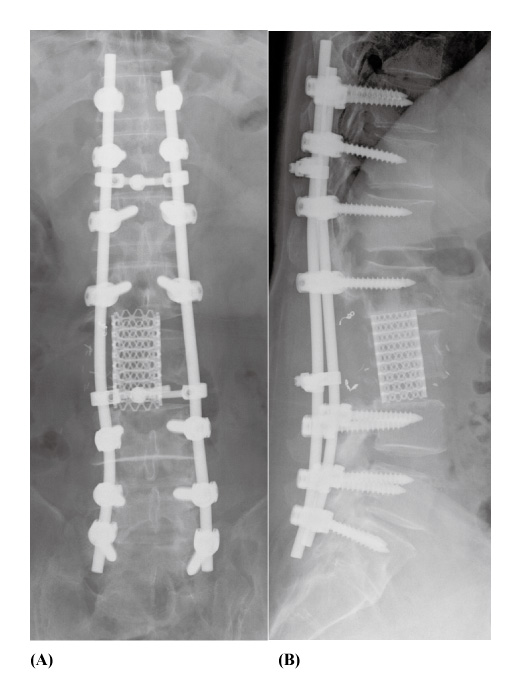
Fig. 5
Postoperative radiographs: anteroposterior (A) and lateral (B) views
However, we had to leave in place the anterior portion of the L3 vertebra because it was too difficult from our lateral approach to access the segmental artery on the contralateral side (Fig. 6). Operative time was 10 hr 23min, and intraoperative blood loss was 10,120g. The pathologic diagnosis of the resected tumor was clear cell carcinoma, which strongly suggests that this tumor was a metastasis from his renal cell carcinoma.

Fig. 6
Postoperative computed tomography(CT)scan at axial view of the L3 level. The anterior portion of L3 vertebra was partial remained (arrows).
The patient’s lower back pain disappeared, and the paralysis of his right leg markedly improved on the day of surgery. He was able to walk with the assistance of a walker eight weeks after surgery, and imaging studies showed no residual tumor nine weeks after discharge. Six months after surgery, he has no back pain, no neurological deficits, and is fully ambulatory. Radiographs show no dislodgement or breakage of the instrumentation, no radiolucent line around the pedicle screws, and maintenance of the spinal alignment (Fig. 7). There is no evidence of metastatic disease or tumor recurrence. (Fig. 8).
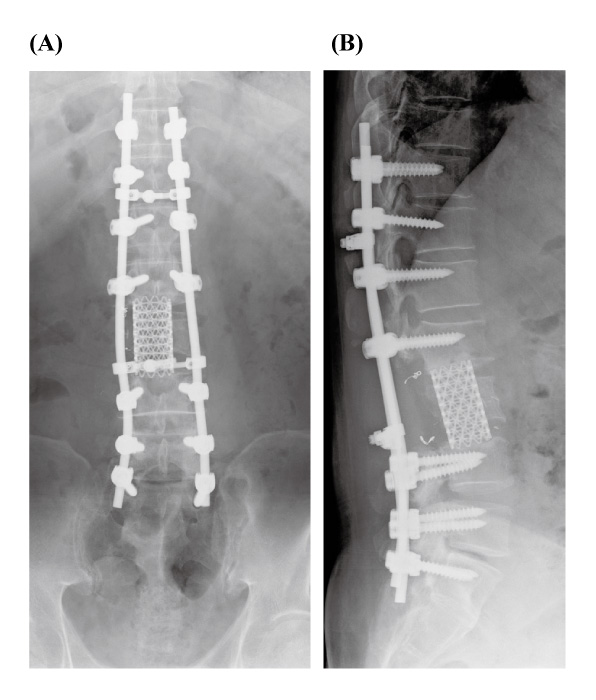
Fig. 7
Postoperative radiographs 6 months after operation: anteroposterior (A) and lateral (B) views. There was no dislodgement or breakage of the instrumentation noted.
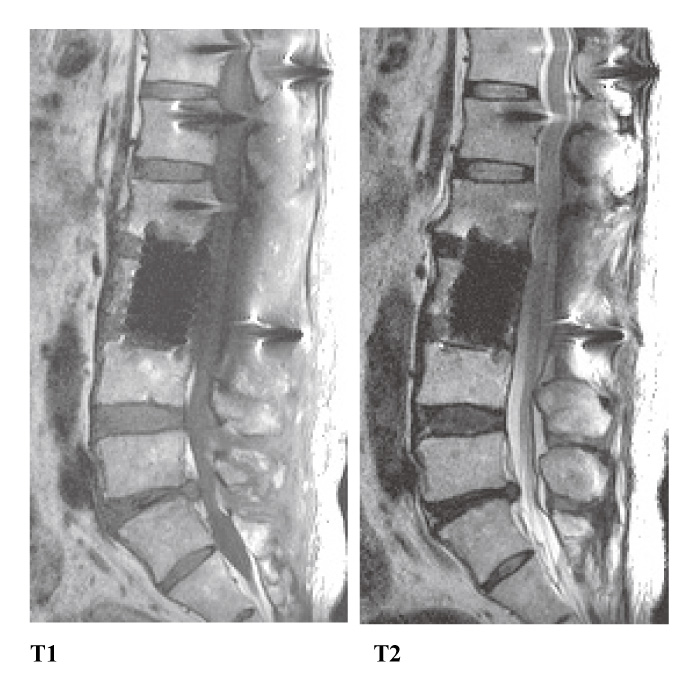
Fig. 8
Postoperative magnetic resonance imaging (MRI) of the lumbar spine. A: T1 of midline sagittal image of the lumbar spine. B: T2 of midline sagittal image of the lumbar spine. The current six months after surgery, metastasis and recurrence has not been confirmed a new, very good decompression and progress.
To recapitulate, a 72-year-old man presented with a solitary metastasis of probable renal origin to the L3 vertebra. We performed TES for the patient via a combined posterior and lateral approach. We were able to resect most of the tumor, and the patient became virtually symptom-free after surgery. However, we were unable to resect the anterior portion of L3 vertebra because of difficulty in accessing the segmental artery on the contralateral side. Because of this difficulty, we would recommend a combined posterior and anterior approach for TES of a lumbar lesion. To determine whether surgical treatment of spinal metastasis is advisable, several scoring systems have been developed[7-9]. Tomita et al. evaluated numerous major and minor prognostic factors for spinal tumors to create a scoring system based on three factors: rate of growth of the primary tumor, number of bone metastases, and the presence and treatability of visceral metastases[7]. Tokuhashi et al. developed a scoring system based on six parameters, which they later revised to take account of the stronger influence of primary tumor type on survival[8,9]. Treatment recommendations are as follows: excisional surgery for patients with a good prognosis (Tokuhashi score of 12-15), palliative surgery for most patients with an intermediate prognosis (score of 9-11), and conservative management for patients with a score of 8 or less[8]. In our patient, we decided on radical surgery because he had a Tokuhashi score of 12 and a Tomita score of 3. Because renal cell carcinomas are normally hypervascular, we embolized the feeding arteries prior to surgery; nonetheless blood loss was greater than 10 liters during surgery. Our experience thus highlights the need to have a plan to manage bleeding during surgery of spinal hypervascular tumors. Kawahara et al. concluded from the cadaveric vascular anatomy of the thoracic and lumbar spines that vertebral tumors involving the upper lumbar spine could be approached by posterior TES[10]. On the other hand, the same authors have recommended a combined posterior and anterior approach for tumors involving lower lumbar levels[11]. Removal of all posterior elements enables dissection of nerve roots at the affected level from neighboring nerve roots, which in turn enables mobilization of the dural tube and facilitates dissection between the ventral surface of the dural tube and the posterior longitudinal ligament or the tumor capsule. The anterior approach enables anterior dissection of the major vessels[11].
In our patient, we selected a combined posterior and lateral approach because we were concerned about possible adhesions of the peritoneum and vessels that might have developed following his prior abdominal surgery to resect a left renal cell carcinoma. We were able to locate and release his aorta, part of the inferior vena cava, and his left segmental artery, which enabled us to resect most of the vertebral body. However, we had to leave in place the anterior portion of the L3 vertebra because we could not access the right segmental artery. Fortunately, MRI and CT revealed metastasis in this case had not invaded into the anterior portion of the L3 vertebra, as no tumor recurrence has occurred up to final follow-up. If TES is performed in lumbar lesion, posterior and an anterolateral extraperitoneal or posterior and an anterior midline transperitoneal approach were recommended based on the current case.
Complications may occur in up to 25% of patients who undergo surgery for spinal metastases, the most common being wound infection[12,13]. Late phase postoperative complications that have been reported include hardware failure, pseudarthrosis, spinal metastases to other levels requiring surgery, and death occurring more than one month after surgery. We encountered no adverse events in our patient, but careful observation was needed during long-term follow-up.
In conclusion, we have presented a case report of a solitary metastasis, probably from a renal carcinoma, to L3. The patient became symptom-free after TES surgery via a combined posterior and lateral approach. However, our combined posterior and lateral approach did prevent us from resecting the anterior portion of the L3 vertebra because of the difficulty in accessing the segmental artery on the contralateral side.
We thus would normally recommend a combined posterior and anterior approach for TES of a lumbar lesion over a combined posterior and lateral approach in cases without any special the circumstances.
72歳男性,第3腰椎への腎癌の転移に対する腫瘍脊椎骨全摘術を試みた1例を経験した。腫瘍は第3腰椎に限局しており,下肢麻痺を呈していたため,後方-側法侵入による腫瘍摘出とインストゥルメンテーションによる固定術を施行した。術前麻痺にて歩行困難であったが,術後独歩可能となった。今回前方からの腎癌摘出の既往から癒着を懸念し,正中アプローチを選択しなかった。しかしながら,側方アプローチでは反対側の分節動脈の処置が困難であり,前方部の健常椎体が一部残存した。腰椎部の腫瘍脊椎骨全摘術を試みる場合の前方アプローチは,前正中よりのアプローチがより望ましいと考えられた。
Department of Orthopaedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
1) Department of Cardiovascular Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
鈴木 都,大鳥精司,井上 玄,折田純久,江口 和,青木保親,石川哲大,宮城正行,新井 玄,鴨田博人,佐久間詳浩,及川泰宏,久保田剛,高相晶士,豊根知明,黒岩璋光,石坂 透1),松宮護郎1),高橋和久: 腰椎腫瘍に対する腫瘍脊椎骨全摘術を試みた1例 -後方,前側法アプローチの問題点-.
千葉大学大学院医学研究院整形外科学
1) 千葉大学大学院医学研究院心臓血管外科学
Tel. 043-226-2117. Fax. 043-226-2116. E-mail: miyako_rush634@yahoo.co.jp
2011年7月11日受付,2011年8月18日受理.
