




Chiba Medical J. 91E:33~37,2015
doi:10.20776/S03035476-91E-6-P33
[ The Chiba Medical Society Award (2015) ]
Masao Koda 1 ) , Takeo Furuya 1 ) , Taigo Inada 1 ) , Koshiro Kamiya 1 )
Mitsutoshi Ota 1 ) , Satoshi Maki 1 ) , Yasushi Ijima 1 ) , Junya Saito 1 )
Kazuhisa Takahashi 1 ) and Masashi Yamazaki 2 )
1) Department of Orthopedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
2) Department of Orthopaedic Surgery University of Tsukuba, Tsukuba 305-8575.
( Accepted September 30, 2015 )
To elucidate neuroprotective effect of granulocyte colony-stimulating factor ( G-CSF ) for acute spinal cord injury ( SCI ) , we performed experimental studies and early phase of clinical trials.
The results of experimental studies showed that G-CSF exerts neuroprotective effects for acute SCI via mobilization of bone marrow-derived cells into injured spinal cord, suppression of neuronal apoptosis, suppression of inflammatory cytokine up-regulation, suppression of oligodendrocyte apoptosis and promotion of angiogenesis.
Next we moved to clinical trial. In a phase I/IIa trial, no adverse events were observed. Then, we conducted a non-randomized, non-blinded, comparative trial, which suggested the efficacy of G-CSF for promoting neurological recovery. We are now preparing a phase III trial to confirm G-CSF treatment efficacy for acute SCI. The current trial will include cervical SCI within 48 hours after injury. Patients will be randomly assigned to G-CSF and placebo groups and evaluated by double blinded manner. Our primary endpoint is changes in American Spinal Injury Association motor scores from baseline to 3 months. Each group will include 44 patients ( 88 total patients ) . After completion of this clinical trial, pharmaceutical approval will be applied for health insurance publication. G-CSF-mediated neuroprotection is a promising candidate for a novel therapeutic approach for SCI.
G-CSF , spinal cord injury , neuroprotection , clinical trial
Acute spinal cord injury ( SCI ) is generally divided into two chronological stages, primary and secondary injury. The primary injury is tissue destruction induced by mechanical stress to the spinal cord. The secondary injury is a pathophysiological reaction of the spinal cord that is triggered by the primary injury. The secondary SCI results in hemorrhage, destruction of the bloodspinal cord barrier, excitotoxicity, electrolyte shift, calcium influx, infiltration of inflammatory cells and an inflammatory reaction dependent upon the release of pro-inflammatory cytokines, all of which can induce cell death resulting in spread of the damaged area. Extensive laboratory and clinical studies have examined mechanisms to suppress the secondary injury because it has the potential to respond to treatment [1] .
Based on the Second National Acute Spinal Cord Injury Study, the administration of high-dose methylprednisolone sodium succinate ( MPSS ) was established as a standard treatment for patients with acute SCI [2] . However, several recent studies have indicated that high-dose MPSS therapy could promote only modest neurological recovery [3] and frequently induces side effects in the respiratory system and digestive organs [4] . Recently published guidelines for SCI revealed that treatment with steroids is not recommended. Therefore, the development of new therapeutic drugs for SCI is greatly needed [5].
Granulocyte colony-stimulating factor ( G-CSF ) is a 19.6-kDa glycoprotein best known as a growth factor for hematopoietic progenitor cells, and is clinically used to treat neutropenia and to mobilize peripheral blood-derived hematopoietic stem cells for transplantation [6 , 7] . Recent experimental studies have indicated that G-CSF also has non-hematopoietic functions and can potentially be used for the treatment of neuronal injury, including stroke and neurodegenerative diseases [8 - 12] .
Thus, we hypothesized that the administration of G-CSF is neuroprotective for acute SCI, and examined this hypothesis using a rodent model of SCI.
To elucidate the effects of G-CSF-mediated mobilization of bone marrow-derived stem cells on the injured spinal cord, we performed in vivo experiments using bone marrow chimeric mice. Bone marrow cells obtained from green fluorescent protein ( GFP ) transgenic mice were transplanted into lethally irradiated C57BL/6 mice. Four weeks after bone marrow transplantation, SCI was induced by a static load ( 20g, 5 min ) at theT8 level. G-CSF ( 200μi>g/kg/day ) was injected subcutaneously for 5 days. Immunohistochemistry for GFP and cell lineage markers was performed to evaluate G-CSF-mediated mobilization of bone marrow-derived cells into injured spinal cord. Hind limb locomotor recovery was assessed for 6 weeks.
Immunohistochemistry revealed that G-CSF increased the number of GFP-positive cells in injured spinal cord, indicating that bone marrow-derived cells were mobilized and migrated into the injured spinal cord. The numbers of double-positive cells for GFP and glial markers were larger in the G-CSF-treated mice than in the control mice. Luxol Fast Blue staining revealed that G-CSF promoted sparing of the white matter. G-CSF-treated mice showed significant recovery of hind limb function compared with control mice.
These results support previous findings that G-CSF showed efficacy for the treatment of SCI through the mobilization of bone marrow-derived cells [13].
To elucidate the anti-apoptotic effect of G-CSF on spinal cord neurons, we performed in vitro and in vivo experiments. The addition of G-CSF suppressed glutamate-induced cell death of cultured cerebellar granule neurons in vitro. Moreover, we used a mouse model of compressive SCI to examine the neuroprotective potential of G-CSF in vivo. Histologic assessment using cresyl violet staining revealed that the number of surviving neurons in the injured spinal cord was significantly increased in G-CSF-treated mice compared with control mice. Immunohistochemistry also revealed that G-CSF suppressed neuronal apoptosis after SCI. Moreover, the administration of G-CSF promoted hind limb functional recovery. Examination of signaling pathways downstream of the G-CSF receptor suggests that G-CSF might promote functional recovery by inhibiting neuronal apoptosis after SCI [14] .
Next, we performed in vivo experiments to elucidate the effect of G-CSF for oligodendrocyte apoptosis after SCI. Contusive SCI was induced in adult female Sprague-Dawley rats using the Infinite Horizon Impactor ( magnitude: 200 kilodyne ) . Recombinant human G-CSF ( 15.0μg/kg ) was administered by tail vein injection at 1 h after surgery and daily the next 4 days. The vehicle control rats received equal volumes of normal saline at the same time points. Real-time reverse transcriptase polymerase chain reaction ( RT-PCR ) and western blot analysis revealed that G-CSF suppressed the expression of pro-inflammatory cytokines ( IL-1 beta and TNF-alpha ) at both the mRNA and protein levels. Histological assessment with Luxol Fast Blue staining revealed that the area of white matter that was spared in the injured spinal cord was significantly larger in G-CSF-treated rats. Immunohistochemical analysis showed that G-CSF promoted the upregulation of the anti-apoptotic protein Bcl-Xl in oligodendrocytes, suppressing apoptosis after SCI. Moreover, G-CSF administration promoted better functional recovery of hind limbs. G-CSF protects oligodendrocytes from SCI-induced cell death via the suppression of inflammatory cytokines and up-regulation of anti-apoptotic proteins. As a result, G-CSF attenuates white matter loss and promotes hind limb functional recovery [15] .
A contusive SCI rat model was used and the animals were randomly allocated to either a G-CSF treatment group or a control group. The integrity of the blood-spinal cord barrier was evaluated by measuring the degree of edema in the cord and the volume of extravasation. For histological evaluation, cryosections were immunostained with anti-von Willebrand factor and the number of vessels was counted to assess revascularization. Real-time RT-PCR was performed to assess the expression of angiogenic cytokines, and recovery of motor function was assessed with functional tests. In the G-CSF-treated rats, the total number of vessels with a diameter > 20μm was markedly larger and the expression of angiogenic cytokines was significantly higher compared with the control group. The G-CSF-treated group showed significantly greater recovery of hind limb function than the control group. G-CSF exerts neuroprotective effects via promotion of angiogenesis after SCI [16] .
To confirm the safety and feasibility of G-CSF administration for acute SCI, we have initiated a phase I/IIa clinical trial of neuroprotective therapy using G-CSF. The trial included a total of 16 SCI patients within 48 h of onset. In the first step, G-CSF ( 5μg/kg/ day ) was intravenously administered for 5 consecutive days to five patients. In the second step, G-CSF ( 10μg/ kg/day ) was similarly administered to 11 patients. We evaluated motor and sensory functions of patients using the American Spinal Cord Injury Association ( ASIA ) score and ASIA impairment scale ( AIS ) grade. In all 16 patients, neurological improvement was obtained after G-CSF administration. AIS grade increased by one step in nine of 16 patients. A significant increase in ASIA motor scores was detected 1 day after injection ( P < 0.01 ) , and both light touch and pin-prick scores improved 2 days after injection ( P < 0.05 ) in the 10-μg group. No severe adverse effects were observed after G-CSF injection. These results indicate that intravenous administration of G-CSF ( 10μg/kg/day ) for 5 days is essentially safe, and suggests that some neurological recovery can occur in most patients. We suggest that G-CSF administration could be therapeutic for patients with acute SCI [17] .
Next we conducted a multicenter prospective, non-randomized, non-blinded, controlled clinical trial to assess the preliminary efficacy and feasibility of G-CSF therapy for patients with acute SCI. The trial ran from August 2009 to March 2011, and included 41 patients with SCI treated within 48 hours of onset. Informed consent was obtained from all patients. After providing consent, patients were divided into two groups. In the G-CSF group ( 17 patients ) , G-CSF ( 10μg/kg/d ) was intravenously administered for 5 consecutive days, and in the control group ( 24 patients ) , patients were similarly treated but did not receive G-CSF. We evaluated motor and sensory functions using the ASIA score and AIS at 1 week, 3 months, 6 months, and 1 year after onset. Only two patients did not experience AIS improvement in the G-CSF group. In contrast, 15 patients in the control group did not experience AIS improvement. In the analysis of ASIA motor score, there was a significant difference between the G-CSF and the control groups in increased ASIA motor score 1 year after SCI ( mean, 30.5 ± 20.8 points in the G-CSF group, 15.7 ± 16.4 in the control group, P < 0.05, ( Fig.1 ) . Despite the study limitation that patient selection was not randomized, the present results suggest the possibility that G-CSF administration has beneficial effects on neurological recovery in patients with acute SCI [18] .
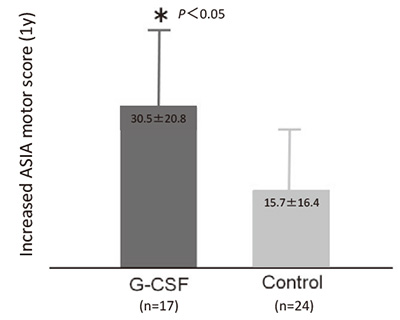
Fig.1
Result of multicenter prospective, non-randomized, non-blinded, controlled clinical trial to assess the preliminary efficacy and feasibility of G-CSF therapy for patients with acute SCI. There was a significant difference between the G-CSF and the control groups in increased ASIA motor score 1 year after SCI(mean, 30.5 ± 20.8 points in the G-CSF group, 15.7 ± 16.4 in the control group, P < 0.05)
Based on the results of basic research and the early phase clinical trial, we planned to perform a prospective, randomized, double-blind, placebo-controlled clinical trial to confirm the therapeutic effects of G-CSF for acute SCI. Our protocol was approved by the Pharmaceuticals and Medical Device Agency and the trial will be funded by the Center for Clinical Trials, Japan Medical Association.
The current trial will include cervical SCI ( severity of AIS B/C ) within 48 hours after injury. Patients will be re-assessed for neurological status at 48 hours after injury, and those whose palsy is AIS B/C will be enrolled. Patients with neurological recovery to AIS D will be excluded. Patients will be randomly assigned to G-CSF and placebo groups. The G-CSF group will be administered 400μg/m2/d G-CSF for 5 days via intravenous infusion in normal saline for 5 consecutive days. The placebo group will be similarly administered a placebo ( Fig.2 ) .
Allocation will be concealed between blinded evaluators of efficacy/safety and those performing the laboratory analysis, because G-CSF markedly increases white blood cell counts, which can reveal patient treatment. Our primary endpoint will be changes in ASIA motor scores from baseline to 3 months after administration. Each group will include 44 patients ( 88 total patients ) .
After completion of this clinical trial, pharmaceutical approval will be applied for health insurance publication. G-CSF-mediated neuroprotection is a promising candidate for a novel therapeutic approach for SCI.
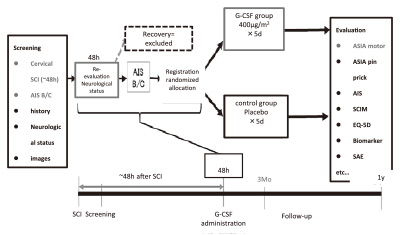
Fig.2
Study design outline of the protocol of a prospective, randomized, double-blind, placebo-controlled clinical trial to confirm the therapeutic effects of G-CSF for acute SCI.
The present work was supported by Grants-in-Aid for Scientific Research from the Ministry of Education, Science and Culture of Japan.
Address correspondence to Dr. Masao Koda.
Department of Orthopedic Surgery, Graduate School of Medicine, Chiba University, 1-8-1, Inohana, Chuou-ku, Chiba, 260-8670 Japan.
Phone: +81-43-226-2961. Fax: 81-43-224-5124.
E-mail: masaokod@gmail.comimpairment
Abbreviations:
SCI ( spinal cord injury ) , G-CSF ( granulocyte colony-stimulating factor ) , MPSS ( methylprednisolone sodium succinate ) , GFP ( green fluorescent protein ) , IL-1β ( interleukin 1 beta ) , TNF-α ( tumor necrosis factor-alpha ) , ASIA ( American Spinal Cord Injury Association ) , AIS ( ASIA impairment scale )
