




Chiba Medical J. 92E:11~14,2016
doi:10.20776/S03035476-92E-2-P11
[ Original Paper ]
Takane Suzuki1), Kazuki Kuniyoshi2), Yusuke Matsuura2), Rei Abe2)
Hitoshi Kiuchi2), Keisuke Ueno2), Tomoyo Akasaka2), Aya Kanazuka1)
Maki Iwase2), Naoya Hirosawa2), Jin Takahashi2), Jun Kakizaki2)
Toshikazu Kunishi2), Kenichi Murakami2), Kouji Sukegawa3)
Nahoko Iwakura4) and Kazuhisa Takahashi2)
1) Department of Bioenvironmental Medicine, Graduate School of Medicine, Chiba University, Chiba 260-8670.
2) Department of Orthopedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
3) Biomechanics Laboratory and Tendon & Soft Tissue Biology Laboratory, Mayo Clinic
4) Department of Orthopedic Surgery, Tokyo Women’s Medical University, Tokyo 162-8666.
(Received October 14, 2015, Accepted October 29, 2015)
Pain reduction effect of vibratory stimulation has been controversial. In previous studies, reseachers evaluated the effect for injection pain. However, as injection procedures differ with the skills of individual doctors, the uniformity of ‘identical’ pain stimulation attempted in these studies remains unverified. In the present study, we used well-controlled electrical stimulation on the pulp of the finger to simulate superficial somatic pain. 24 healthy subjects were studied. In each trial, 50-mA electrical stimulation was applied for 2 ms on the middle finger. We compared three trials: without vibration, with vibration on the ipsilateral metacarpophalangeal joint and with vibration on the contralateral metacarpophalangeal joint. Statistical analysis was performed using the Wilcoxon signed-rank test for comparison. The trial of vibration on the ipsilateral metacarpophalangeal joint showed a significantly lower minimum pain score, implying positive effects of vibratory stimulation.
vibration, superficial somatic pain, electrical stimulation, injection, anaesthesia
Vibratory stimulation has been reported to be effective for pain reduction in various clinical areas, including dentistry[1], dermatology[2,3], ophthalmology[4]and plastic surgery[5]. Conversely, one study reported vibratory stimulation as not being effective for corticosteroid injection for trigger finger[6]. However, the previous studies were not uniform and varied in terms of the injection procedures, such as injection speed and depth.
In addition, the results may be influenced by the intensity of rubbing for sterilisation or general sedation, which were not considered in the previous studies. Some authors attempted to administer the same pain stimulus; however, as injection procedures differ with the skills of individual doctors, the similarity of the extent of pain in these studies remains unverified. The definition of pain associated with injection is also ambiguous and can include pain associated with the puncture itself or pain associated with the pressure generated on fluid injection. In the current study, we evaluated the pain reduction effect of vibratory stimulation in healthy subjects using well-controlled electrical stimulation.
To determine an appropriate sample size, we selected a 2-point change in the Numeric Rating Scale (NRS) with a standard deviation (SD) of 2.5 points as clinically significant[4,7]. A sample size of at least 19 hands was needed when a power calculation with 90% power and P=0.05 was adopted. One hand each of 24 healthy subjects was included in the present study. They were given an information sheet explaining the aim of the study without describing the specific effects of the vibrating device and placebo to reduce the risk of biased perception. Institutional review board approval was received at our institution.
The electrically stimulated side was randomly selected in each subject. A bipolar electrical stimulator (Neuropack S1, Nihon Kohden, Tokyo, Japan) was placed on the distal pulp of the middle finger without rubbing. Electrical stimulation of 50 mA for 2 ms was applied in each trial. Prior to electrical stimulation, a vibrator (Handy massager, Yamazen Corp, Osaka, Japan) was applied to provide a 108-Hz vibratory stimulus. The subjects were asked to close their eyes before each trial to blind subject visual information and were allowed to open their eyes after vibration was stopped.
The experimental protocol is shown in Fig. 1. There were three types of trials. In Trial 1 (T1: sham procedure), we used two vibrators, with both the vibrators placed in close proximity. Electrical stimulation was applied with actual contact of a switched-off vibrator at the ipsilateral palmar side of the metacarpophalangeal joint (MPJ). Simultaneously, vibration sound was generated for 5 s with another switched-on vibrator, which was not touching the hand (Fig. 2). Electrical stimulation was applied 4 s after starting the vibratory sound, which the subjects could hear from the second vibrator. In Trial 2 (T2), electrical stimulation was applied with contact of the vibrator at the ipsilateral palmar side of the MPJ. Vibration was applied for 5 s, and electrical stimulation was applied 4 s after the vibration started. In Trial 3 (T3), electrical stimulation was applied with contact of the vibrator at the contralateral palmar side of the MPJ. No sedation was given for any experiment. To avoid the effects of stimulation sequence, the 24 subjects were randomly divided into six groups depending on the sequence of trials: T1-T2-T3, T1-T3-T2, T2-T1-T3, T2-T3-T1, T3-T1-T2 and T3-T2-T1.
There was at least a one-minute interval between the trials. NRS was used for pain evaluation-a score of zero means ‘no pain’ and ten means ‘worst pain’. The NRS score of electrical stimulation was defined as PS1 in T1, PS2 in T2 and PS3 in T3. The data was evaluated as follows: the average pain score in each trial; the average improvement between PS1 and PS2 or between PS1 and PS3; and the number of subjects who reported a 2-point or more reduction between PS1 and PS2 or between PS1 and PS3 after vibration.
Statistical analysis was performed using the Wilcoxon signed-rank test for comparison. A significance level of P<0.05 was used to assess statistically significant differences.
Fig.1
The experimental protocol:
Refer to“ Experiments” in Method.
EC: Eye closed; S: stimulation; R: record; MPJ: volar side of metacarpophalangeal joint of the middle finger
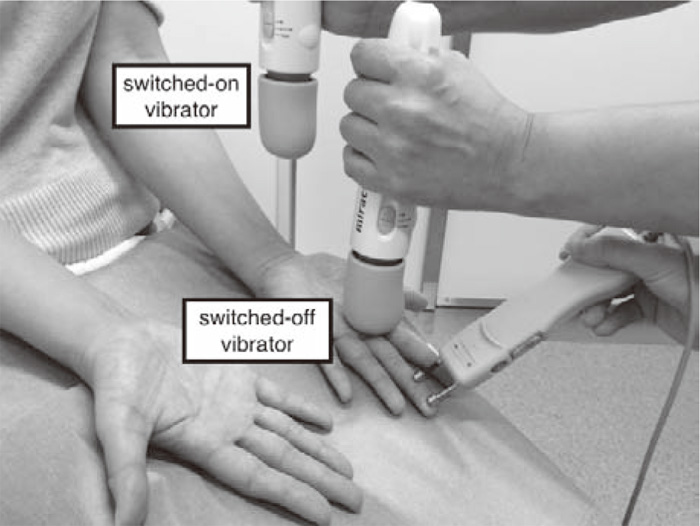
Fig. 2
Sham procedure. One switched-off vibrator was placed on MPJ and another one provided only vibration sounds at the same time.
In the 24 participants (men, 16; women, 8; average age, 29.2 years, age range, 22-42 years), the average PS1 was 6.5 (SD 1.7), PS2 was 4.0 (1.7) and PS3 was 5.6 (2.0). Significant differences were noted between PS1 and PS2 and between PS2 and PS3. The average improvement score of PS1-PS2 was 2.5 (1.1) and that of PS1-PS3 was 0.9 (0.9). Compared with PS1, a 2-point or higher reduction was recorded in 21 of 24 (88%) hands in PS2 and in seven of 24 (29%) hands in PS3. No adverse effects related to the procedures were noted.
Table.1
NRS score in each trial( n=24)
Table.2
Comparison of pain score between trials( n=24)
Pain reduction using vibration has been reported in various clinical settings. Nasehi et al.[8]reported significant pain reduction using intraoral vibratory stimulation during nerve block. In that study, two surgeons used identical devices for injections. However, there were no further detailed descriptions about the procedures, such as injection depth, angle, or speed. Nanitos et al.[9]reported significant pain reduction with vibration during infiltration injection and nerve block injection; however, there was insufficient information about the procedures. Park et al.[6]reported on the use of vibration for pain reduction during corticosteroid injection for trigger finger. They compared the extent of pain caused by injection under the following three conditions: with 95-Hz vibratory stimulation, with ultrasound vibration and without vibration. They did not find significant differences among the three procedures and concluded that it may be due to the depth of the target tissue. The tendon sheath is located in a relatively deep, confined space. Therefore, injection may cause pressure increase in the tendon sheath, which may induce a type of pain different from that caused by superficial injection. They considered injection depth could be an important factor in the pain reduction effects of vibration. In the current study, we used superficial electrical stimulation to avoid the influences of injection depth or increased pressure. We were able to apply identical and constant stimulation and demonstrated positive effects of vibratory stimulation.
However, there may be some issues regarding the feasibility of using electrical stimulation to evaluate the intensity of pain experienced by the patients. By using electrical stimulation as a measure, Ohotori et al.[10]attempted to evaluate the intensity of lower back pain, although no skin puncture was involved in this study. They concluded that the intensity of electrical stimulation, given as pain, correlated with the McGill Pain Questionnaire or Numeric Rating Scale, which are widely used for the evaluation of lower back pain. To our knowledge, previous reports used actual needle injection, which may lead to variation in parameters, such as injection speed, angle and/or depth. At present, to the best of our knowledge, no other procedure for adequate stimulation is available except electrical stimulation. Further neurophysiological studies are warranted.
The authors are very grateful to our biostatistician, Kengo Nagashima.
Address correspondence to Dr. Takane Suzuki.
Department of Bioenvironmental Medicine, Graduate School of Medicine, Chiba University, 1-8-1, Inohana, Chuou-ku, Chiba, 260-8670 Japan.
Phone: +81-43-226-2017. Fax: +81-43-226-2018.
E-mail: takane.suzuki@faculty.chiba-u.jp
