




Chiba Medical J. 92E:37~41,2016
doi:10.20776/S03035476-92E-5-P37
[ Original Paper ]
Michiaki Miura1), Junichi Nakamura1), Makoto Otsuka2)
Takayuki Nakajima3), Munenori Takeshita2), Yasushi Wako1,2)
Shuichi Miyamoto1), Fumio Hasue2), Takayuki Fujiyoshi2), Ryo Hiwatari2)
Kazuhisa Takahashi1), Seiji Ohtori1), Sumihisa Orita1), Takane Suzuki4) and Tadashi Tanaka2)
1) Department of Orthopedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
2) Department of Orthopedic Surgery, Kimitsu Chuo Hospital, Kisarazu 292-8535.
3) Department of Orthopedic Surgery, Eastern Chiba Medical Center, Togane 283-8686.
4) Department of Bioenvironmental Medicine, Graduate School of Medicine, Chiba University, Chiba 260-8670.
(Received June 3, 2016, Accepted July 11, 2016)
Objective: The aim of the study is to document the outcome of osteosynthesis with locking plate and cable for periprosthetic femoral fracture(PFF).
Patients: Between 2007 and 2014, nine patients were identified: five with Vancouver type B1 fracture, one with type B2, and three with type C. A single lateral locking plate and cables were used for osteosynthesis in all patients. Cerclage also was used to gain tight fixation depending on the fracture type. The rate and the time of fracture union, walking ability at final follow-up, the position of the fracture reduction at the time of surgery, and complications of surgery were investigated.
Results: Patients achieved fracture union on average by 6.5 months after fixation. At mean follow-up of 14 months, 7 of 9 patients had recovered their pre-injury walking ability. Two patients still had a fracture gap of 4mm after fixation, one had stem subsidence of 5mm one month after fixation, and another had delayed-union. There were no serious complications such as infection or hardware failure.
Conclusion: The outcome of osteosynthesis with locking plates and cables for PFFs was successful. The degree of reduction and strong fixation are essential factors for the treatment of periprosthetic femoral fractures.
osteosynthesis, Vancouver classification, periprosthetic femoral fracture, locking plate, cable
Periprosthetic femoral fracture(PFF) is a serious complication after total hip arthroplasty(THA) and hemiarthroplasty. The number of PFFs is increasing because of an aging society and the increase of hip arthroplasties, and this trend will continue to rise in the future. The incidence of PFF is estimated to be about 1% after primary hip joint arthroplasty and up to 4% after revision arthroplasty[1]. The risk factors of PFF are female gender, advanced age, posttraumatic osteoarthritis, developmental dysplasia of the hip, osteoporosis, and rheumatoid arthritis [2,3]. Because of the presence of the stem in severely osteoporotic bone, the treatment of PFFs is technically demanding. According to the Vancouver classification, osteosynthesis is recommended for type B1 and type C fractures[4]. While many options are available for improving the outcome of osteosynthesis, the best method of treating PFFs is still controversial.
The aim of this study is to document the outcome of osteosynthesis with locking plates and cables for PFFs.
Between April 2007 and March 2013, thirteen patients with Vancouver type B and type C periprosthetic femoral fractures were referred to our institution. We excluded three Vancouver type B1 fractures with conservative treatment and one Vancouver type B1 fracture which was operated but dropped out early in the follow-up. We included the remaining nine patients(two males and seven females), who were treated operatively. The fracture involved five right femurs and four left femurs. There were five Vancouver type B1 fractures, one type B2 fracture and three type C fractures. All fractures also were classified by the AO(Arbeitsgemeinschaft Osteosynthese fragen) / OTA(Orthopaedic Trauma Association) classification:there were three type 32-A1 fractures(simple spiral fractures), three type 32-A2 fractures(simple oblique fractures), one type 32-A3 fracture(simple transverse fracture) and two type 33-A1 fractures. All occurred after primary hip joint arthroplasty; five after cementless hemiarthroplasty, two after cement hemiarthroplasty, one after cementless THA, and one after cement THA. All participants were injured by low-energy falls from a standing position, and all were closed fractures without any associated injuries. The mean time from arthroplasty to periprosthetic fracture was 5 years and 8 months(range from 1 year and 1 month to 13 years and 2 months). The mean age at fracture was 76 years.
Osteosynthesis was performed for all patients using a lateral approach with a less invasive procedure that avoided unnecessary dissection of muscle and skin. In Vancouver type B fractures, reversed LCP-DF(Synthes, Paoli, PA, USA®)) was used for five patients and LCPbroad(Synthes, Paoli, PA, USA®) was used for one patient. Cable fixation was added to plate fixation for all six patients. In Vancouver type C fractures, LCPDF was used for all three patients and cable fixation was added for one of the three patients. Cerclage with Nesplon cable(Alfresa, Osaka, Japan®), which is a radiolucent fiber product that keeps the reduced position firmly without obstructing the view of the fracture gap by fluoroscopy, also was used before plate fixation depending on the fracture type. Bone graft was not used in any cases. Partial weight bearing was allowed four to six months after surgery, and full weight bearing was allowed eight months after surgery. The mean follow-up period was 14 months.
We retrospectively studied the postoperative reduction and bone union by radiological evaluation, the change of walking ability by clinical evaluation, and assessed postoperative complications. Postoperative reduction depended on the AO/OTA classification. For AO/OTA type 32 fractures, the fracture gap between the outer cortices of the fracture site was measured on the postoperative X-rays. For AO/OTA type 33 fractures, the femoral angle was defined as the angle between the axis of the femur and the distal articular surface of the femur(normal range 75-85°). We defined bone union clinically as full-weight walking ability without pain, and defined radiographic union by bone bridging more than two cortices on X-rays[5]. Walking ability was classified into four groups: walking independently, walking with a cane, walking with a walker, and sitting on a wheel chair. All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. For this type of study formal consent is not required.
The mean operative time was 146 minutes(range from 119 to 191 minutes), and the mean blood loss was 213ml(range from 64 to 439 ml). The mean length of hospitalization was 42 days(range from 15 days to 81 days).
In AO/OTA type 32 fractures(n=7), the fracture gap was zero with anatomical reduction in five patients, 4mm to the axial direction in one patient and 4mm posterior in one patient. In AO/OTA type 33 fractures(n=2), the femoral angles were 77° and 83° respectively, achieving good alignment. Bone union was achieved in a mean of 6.5 months(range from 2.5 months to 12 months).
Seven of nine patients recovered the same walking ability as they had prior to surgery. Walking ability worsened because of heterotopic ossification around the hip joint in one case, and old age(96 years) in one case.
There were no infections, dislocations of the hip or implant failures. Delayed-union was found in one case: an 85-year-old woman with a transverse fracture just below the cement stem(Fig. 1) and 5 mm stem subsidence was found in one case: a 66-year-old man, initially diagnosed with a Vancouver type B1 fracture and operated with an osteosynthesis, appeared postoperatively to be a type B2 fracture (Fig. 2). No revision operation was required and finally they achieved bone union and were able to recover their ability to walk as they could before surgery.
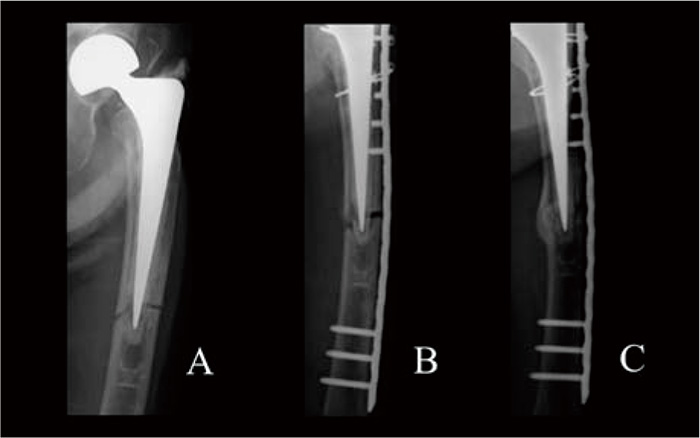
Fig.1
The fracture gap was so small that we performed minimally invasive plate osteosynthesis(MIPO), but the fracture gap was widened during the surgery and it took 12 months to obtain bone union. Finally she recovered her walking ability.
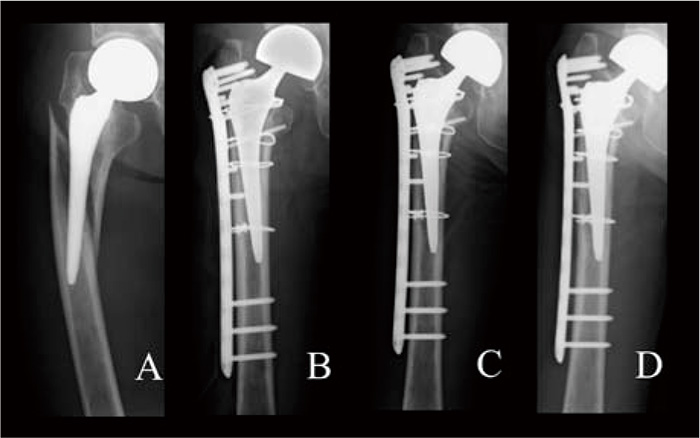
Fig.2
The fracture gap remained intraoperatively and stem subsidence was found one month after the operation. No more subsidence occurred after that, and the patient could walk independently without pain. Bone union was achieved 4.5 months after the operation.
The treatment of PFFs is challenging because of the presence of the stem in severely osteoporotic bone. Several fixation devices are available for the treatment of PFFs, including conventional and locking plates, which are used either alone or in combination with strut bone graft, cable and cerclage[6,7]. A complication rate of 33% including hardware failure, nonunion, and new fracture was reported after treatment with conventional plate-screw systems, resulting in a poor outcome in 57% of cases[8]. In general, successful clinical results have been reported for locking plate fixation. Locking plates provide angular stability to the fracture fixation and tend to maintain periosteal blood supply. Biomechanical studies demonstrate that locking plates provide superior stability compared to conventional plates[9]. But current literature suggests that the clinical results of osteosynthesis for PPFs with locking plates are not superior to other fixation methods[10]. This result occurred because the study included all cases treated with locking plates without considering the reduced position, severity of osteoporosis and fracture pattern, invasive surgical procedures, or the use of bicortical screws or cables. Moreover, there is a selection bias because locking plates tend to be used for more difficult fractures including previous revision cases that have resulted in poor outcomes[11]. We hypothesized that anatomical reduction and strong fixation with a locking plate and cables would lead to bone union and full recovery of pre-operative walking ability.
The good reduction is the most important factor for treating PFFs because the degree of fracture reduction affects the stability of the whole construct and the bending behavior of the fixation that can result in implant failures[12]. However, there have been many clinical series that did not emphasize the importance of reduction[7,9,11]. On the other hand, invasive surgical procedures that involve unnecessary dissection of muscles and skin damage the periosteal blood supply, even when using a locking plate, and can cause more frequent infections and delayed- or non-unions. Biomechanical studies have shown that a locking plate with monocortical screws and cables provides stronger fixation than with screws or cables alone[13]. Reversed LCP-DF is useful for PFFs because it is long enough to cover most of the whole femur, and a maximum of seven screws can be inserted in the proximal region to create a stronger fixation. Recent literature has shown that the use of proximal bicortical screws also provides strong fixation[13,14]In our study, there was one patient with delayed-union due to poor reduction with minimally invasive plate osteosynthesis(Fig. 1). A better reduction might have prevented the delayed union.
Another prognostic factor for stem loosening was the misinterpretation of Vancouver type B2 fracture as type B1. A previous study showed that interobserver and intraobserver reliability and validity of the Vancouver classification are low, and this misinterpretation caused complications. Both preoperative and intraoperative assessment of stem stability were recommended[15,16]. In general, revision THA is recommended for treatment of Vancouver type B2 fractures, but problems can occur with revision THA. Compared with osteosynthesis, revision THA generally requires a longer operative time, involves more blood loss, and has more complications, such as a 50% incidence of stem subsidence, new fractures, and infections[17,18]. In this study, while preoperative X-rays, a CT scan and intraoperative assessment of the stem loosening were carried out, the fracture gap remained intraoperatively and the stem subsidence was found postoperatively in one case(Fig. 2). It is extremely difficult to identify Vancouver fracture types correctly, and difficult to determine whether an anatomical reduction can be achieved. Fortunately, bone union was achieved and the clinical outcome for this patient was acceptable due to good reduction and firm fixation. When it is uncertain whether stem loosening exists, revision THA is not favorable. It is important to carefully achieve the anatomical reduction, and to perform osteosynthesis with strong fixation devices. While the Vancouver classification is widely accepted for decision making in treating PFFs, an osteosynthesis in combination with a locking plate, cable system and cerclage may be indicated in these mixture cases of Vancouver type B1 and B2 fracture.
There are several limitations to this study. First, this is a retrospective study with a very small number of patients. Second, there were no control groups to compare with other fixation methods. Further study is needed to determine the best treatment for this intractable fracture.
In conclusion, we reported successful treatment of PPFs with locking plates and cables. Proper anatomical reduction and strong fixation are predictive factors in the successful outcome of PFF treatment.
Abbreviations:Periprosthetic femoral fracture(PFF), total hip arthroplasty(THA), AO(Arbeitsgemeinschaft Osteosynthese fragen), OTA( Orthopaedic Trauma Association)
Address correspondence to Dr. Junichi Nakamura.
Department of Orthopedic Surgery, Graduate School of Medicine, Chiba University, 1-8-1, Inohana, Chuou-ku, Chiba, 260-8670 Japan.
Phone: +81-43-226-2117. Fax: +81-43-226-2116.
E-mail: njonedr@chiba-u.jp
