




Chiba Medical J. 94E:25-31,2018
doi:10.20776/S03035476-94E-3-P25
[ Original Article ]
Yorihiko Muto, Hideaki Miyauchi, Gaku Ohira, Koichi Hayano
Kazuo Narushima, Kazufumi Suzuki and Hisahiro Matsubara
Department of Frontier Surgery, Chiba University Graduate School of Medicine, Chiba 260-8670.
(Received January 17, 2018, Accepted March 15, 2018)
Background/Aims: This study is to establish the method to assess anastomotic blood flow using NIR-ICG AG.
Methods: Sigmoid colectomy and anastomosis of a pig was performed, and the anastomotic staining pattern after clamp and declamp of superior rectal artery was visually classified into four categories of vessel staining pattern classification system(VSPCS). Then, in 7 patients who underwent left colectomy, the anastomotic perfusion parameters including staining start time, peak staining value, time to peak staining, and staining value after 5 seconds were calculated using ImageJ software, and staining pattern was also classified by VSPCS.
Results: According to the pig study, four classifications by vessel stain pattern. In human study, 7 rectal cancer patients received transanal NIR-ICG AG. Anastomotic leakage was observed in two patients, whose anastomotic VSPCS was all categorized as C2, while the patients that were categorized as C3-4 didn’t show anastomotic leakage. However, no perfusion parameters quantified by image J were associated with anastomotic leakage. VSPCS significantly reflected the results of anastomotic leakage.
Conclusions: Our classification of anastomotic VSPCS for NIR-ICG AG allowed for the more accurate prediction of anastomotic leakage.
ICG, fluorescence imaging, anastomotic blood flow, anastomotic leakage
Anastomotic leakage is the most severe complication of intestinal surgery. The suture failure rate in rectal surgery is higher than that at other sites of the colon. In Japan, the rate is reported to range from 12.4 to 15.3% [1]. Anastomotic leakage may occur for a variety of reasons, including blood flow, tension and the surgical techniques that are applied. The most significant cause is blood flow of the anastomotic site. Recently, it has been reported that intraoperative near-infrared indocyanine green fluorescence angiography(NIRICG AG) would be useful for evaluating the intestinal blood flow[2-4]. ICG is an infrared fluorescent dye that absorbs light between 790 and 805 nm and re-emits it with an excitation wavelength of 835 nm[5,11]. The half-life of ICG is 3-5 min, and it is eliminated by the liver in 15-20 min. The fluorescence emitted by ICG can be captured to a depth of 1-2 mm. Recently, several studies have presented a novel method involving intraoperative ICG angiography and <5% iodide sodium for sensitively detecting the blood flow in the coronary arteries and bypass grafts during CABG.[6-11]; and therefore, it would be also useful to assess blood flow of the anastomotic site. However, the evaluation method for intestinal blood flow using NIR-ICG AG has not been established yet. It is still largely depending on the experience of the operator. Another problem of NIRICG AG is the approach method to evaluate intestinal blood flow of the anastomotic site. It is often difficult to observe the entire circumference of the anastomotic site simultaneously from the extraluminal(abdominal) approach due to the limitation of observation area. We hypothesized that intraluminal(transanal) approac would be a better approach to observe the anastomotic perfusion, because this approach can allow for a simultaneous observation of the entire circumference of the anastomoti site and surrounding capillaries, which enables better observation of anastomotic perfusion using NIR-ICG AG. To date, there are no reports comparing the approaches for NIR-ICG AG to evaluate blood flow of the anastomotic site. Thus, the purpose of this study is to establish the evaluation method for the anastomotic blood flow, and to compare the intraluminal approach with the extraluminal approach using NIRICG AG in colorectal surgery.
This study was conducted in accordance with the ethical principles of the Declaration of Helsinki, and was approved by the institutional review board at Chiba University Hospital. For animal experiment, one male pig weighting 60 kg was studied. For human study, a total of 7 patients(48-77 years, 5 men and 2 women) who received curative surgery for their colorectal cancers in Chiba University Hospital from June 2015 to December 2015 were enrolled in this study. All patients were required to provide written informed consent before study participation. Patients were eligible for enrollment if they were over 18 years old and were scheduled for a left colectomy.
A prototype NIR laparoscopic system(Olympus, Tokyo, Japan)[7]was used in both the transanal and the abdominal approaches. The laparoscopic camera image can be switched from laparoscopic CI to NIR imaging using a lever. The excitation barrier filter only admits light with a wavelength of >800 nm. The NIR camera displays all fluorescent structures in green against a black(non-fluorescent) background. ICG has a peak emission of 830 nm when assessed with NIR light. ICG dye(0.2 mg/kg body weight per image sequence) was injected intravenously and flushed through with 10 ml of saline.
Sigmoid colectomy of a pig was laparoscopically performed. The inferior mesenteric artery (IMA) and the superior rectal artery(SRA) were preserved, and approximately 10 cm of the marginal artery of the sigmoid colon was ligated using a sealing system. Thereafter resection was performed at the most anal side of the colon. Anastomosis was performed using the double stapling technique(DST). First, we clamped the SRA, and ICG(4 mg/kg body weight per image sequence) was intravenously injected, and we observed staining of vessels from intraluminal(transanal) and extraluminal(abdominal) approaches(Fig.1). After declamp of SRA, we observed how staining pattern of anastomosis changed after reperfusion of SRA. When the SRA was clamped, the anastomotic wall appeared black. After declamp of SRA, vascular shadows was observed after approximately one minute(Fig.2). According to the change of the vessel staining pattern after reperfusion of SRA, we categorized the vessel staining pattern of anastomosis. Good blood flow is characterized by a black background and white blood vessels. If the blood flow is poor, the background becomes white. When it becomes even worse, the blood vessel outlines became unclear.
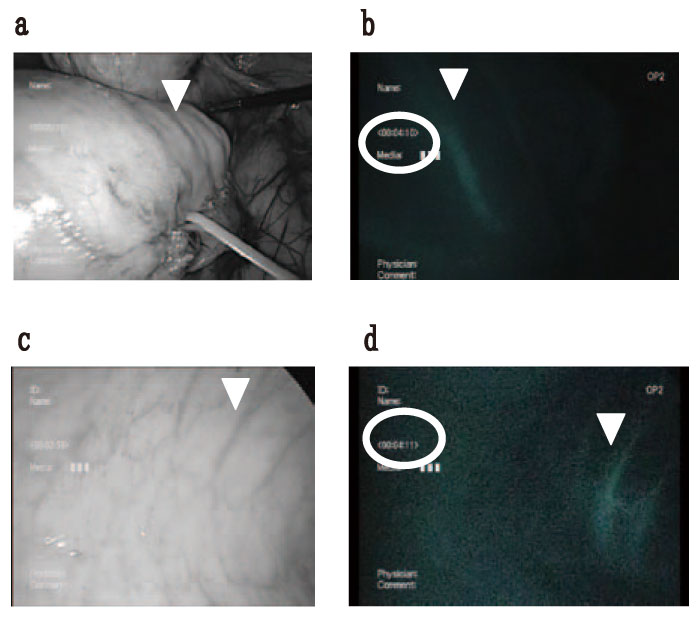
Fig. 1 An NIR perfusion assessment in a Pig undergoing laparoscopic low anterior resection.
We compared the two approaches simultaneously (the same time is shown in the red circle) in the pig experiments. The arrow indicates the same artery of the marginal colon. a/b: Laparoscopic view. c/d: Transanal view.
a. The laparoscopic view under normal light. The SRA is taped.
b. The laparoscopic view under near-infrared fluorescence. Good blood flow of the marginal artery can be confirmed.
c. The transanal view under white light.
d. The trans-anal view under near-infrared fluorescence. Good flow of the capillaries can be confirmed.
b/d. It was compared to the same vessel with the arrow from both approaches using the Image J software program. The gray value of the transanal approach is 77 and abdominal approach is 45.
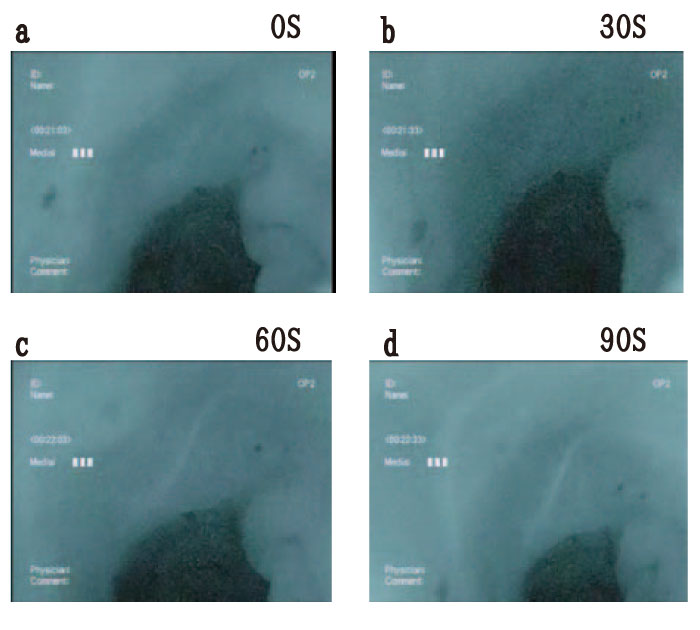
Fig. 2 Near-infrared fluorescence showed changes after the release the clamped SRA(transanal view).
a. The blood vessels under clamping SRA cannot be observed on a white background.
b. At approximately 30 seconds after the release of the clamp, the vessels still cannot be detected.
c. At approximately 60 seconds after the release of the clamp, a thick white blood vessel is observed on the white background.
d. The blood vessels gradually became clearer and could be clearly observed at 90 seconds.
We evaluated the blood flow of the site of anastomosis intraoperatively by ICG infrared fluorescence observation using the intraluminal approach(transanal route) in 7 patients who underwent left colectomy. One patient received sigmoid resection, 4 high anterior resection, and 2 low anterior resection.
A normal endoscope was used to check the hemostasis of the anastomotic site and an air leak test was performed. A fluorescence camera was then inserted via the intraluminal(transanal) approach. ICG is injected after positioning the camera to capture the whole anastomotic site in a single field of view. We observed and evaluated the capillaries on the mucosal surface around the anastomotic site. The region of interest was set on the vessels near the anastomosis.
On the other hand, the staining intensity have been quantified using the Image J software program(ver. 1.39s; National Institutes of Health, available at http:// rsb.info.nih.gov/ij). the Image J software was used to quantify the following 4 perfusion parameters: ① The time to visually confirm the start of dyeing after injected intravenously; ② the time from the start of staining to the peak; ③ the peak staining value; ④ the value that was reached in 5 seconds(Fig.3).
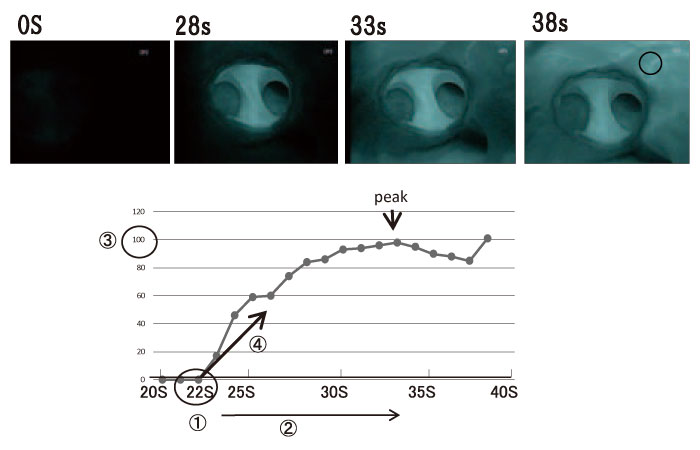
Fig. 3 The Image J software program was used to evaluate the 4 items in the black circle, which indicates an anastomotic site that was confirmed to have good blood flow.
①The staining start time was 22 seconds.
②The peak staining value(100) was achieved at 34 seconds
③The time from the start of staining to the peak of staining was 12 seconds
④Staining value at 5 seconds after the start of the staining, the staining value was 60.
First, according to the SRA reperfusion experiment of the pig, the vessel staining pattern was categorized to four classifications as following: C1, the whole region is black(when SRA clamped), the blood vessels cannot be observed on the black background; white branches of the capillaries can be observed on a black background; C2, thick white blood vessels cannot be observed on the white background; C3, thick white vessels can be observed on a white background; C4, white branches of the capillaries can be observed on a black background (Fig.4). In the comparison between the intraluminal (transanal) and the extraluminal (abdominal) approaches, the view from the intraluminal approach was superior to from the extraluminal approach for evaluating the blood flow in the fine capillaries, because fine capillaries branches of submucosa in the intestine could be observed under the intraluminal approach. A same vessel was quantitatively evaluated from both approaches using the Image J software program. The gray value of the vessel from the intraluminal approach is 77 and that from the extraluminal approach is 45, and thus, the gray value of the same vessel from the intraluminal approach is higher than the extraluminal approach. Therefore, NIR-ICG AG with intraluminal approach allowed for the detailed observation of the anastomotic blood flow(Fig.1).
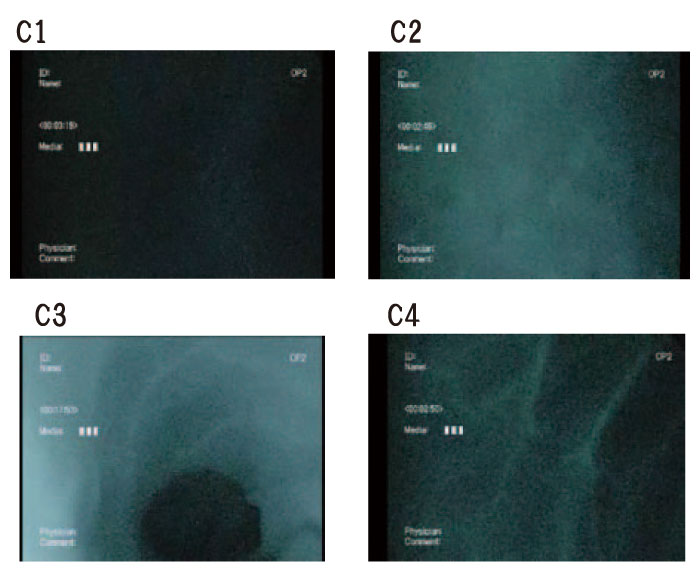
Fig. 4 The changes reflecting blood flow over time(Class 1-4).
a. C1: There is no inflow of arterial blood, the area remains black.
b. C2: The whole area is white, blood vessel shadows are unclear. The whole image has a cloudy appearance.
c. C3: The background of the whole image is white, which reflects mild venous stasis.
d. C4: The background of the image is black and the white branches of the capillaries can be observed.
Based on animal study, intraluminal(transanal) approach was applied to the human study. NIR-ICG AG was performed in 7 patients who underwent left colectomy due to colorectal cancers. Patient characteristics, the NIR-ICG AG evaluation result and postoperative course are given in Table 1 and predictive risk factors for suture failure are given in Table 2. This observation was performed after the completion of anastomosis during surgery. As Case 1 is shown in Figure 3, staining was observed from approximately 22 seconds after the administration of ICG. C4 could be observed after approximately 38 seconds, which confirmed that good anastomotic blood flow had been achieved. As shown in Table 1, suture failure was detected in 2 cases, and these 2 cases were categorized as C2. Whereas, the patients that were categorized as C3-4 were discharged on schedule without anastomotic leakage. Thus, C2 indicated that anastomotic leakage had occurred. The hospitalization period of the two patients with suture failure was extended to approximately one month(Table 1). Figure 3 is an example of quantitative measure of four perfusion parameters using Image J software. The evaluation of the four perfusion parameters using the Image J software program could not predict the leakage. Our vessel staining pattern classification system(VSPCS) was compared with perfusion parameters measured by the Image J, and only VSPCS showed a statistically significant difference to predict anastomotic leakage(0.0476; Table 2).
Table1 summarizes the characteristics of the 7 patients. Postoperative anastomotic leakage occurred in two patients who had no relevant medical history. The other five patients all had relevant medical history, however, the anastomotic blood flow was good(C2 by transanal NIR-ICG AG). The other side shows the details of the two patients with leakage without good blood flow(C3-4).
A comparison of the results between the two groups stratified by the presence or absence of good anastomotic blood flow. The patient characteristics and evaluation methods are also shown. There were no significant differences in the sex, age or the Image J evaluation results. The FVC method showed significant differences in the patients with suture failure.
Anastomotic leakage is the most severe complication of intestinal surgery.[1]NIR-ICG AG has been reported to be useful for in vivo assessment of blood flow [2-4], but the approach and the quantitative method have not been established. In the pig experiment, we demonstrated that intraluminal(transanal) NIR-ICG AG was better for the real-time intraoperative assessment of anastomotic perfusion than extraluminal approach, because it allowed for more stable and wider observation of the anastomotic site. This approach enables better visualization of the anastomotic blood flow. Besides, we defined a new NIR-ICG AG classification system according to staining pattern that could be implemented intraoperatively. Regarding this classification system, we speculated that each classification of staining pattern could indicate following perfusion conditions based on the pig study: C4 indicated good blood circulation(straight artery + observable branches); C3 classification indicated mild venous stasis with arterial circulation(white background + observable straight artery); C2 indicated a lack of inflow of arterial blood, a state in which circulation has stagnated(white background + observed failure in a straight artery); and C1 indicated hemostasis(black).
In the human study, the suture failure was observed in two cases, and they were all classified as C2, while the other five cases with no anastomotic leakage were all categorized C3 or 4. Whereas, Image J-based conventional quantitative measures for anastomotic perfusion were not associated with the clinical results, and it might be because of instability due to the distance and angle between the camera and the object, which could have an influence on the quantification of luminosity. Therefore, the evaluation of anastomotic perfusion with use of the form of the vessel staining can be a more suitable method. According to our classification system, a normal postoperative course could be expected in patients classified as C1 or C2, but colostomy would be recommended for patients classified as C3 or C4. Our new classification system would prevent the delay of discharge, and it can lead to patients’ benefit by reducing the incidence of complications and enabling early hospital discharge and early initiation of adjuvant treatment for better outcome.
We found a useful simple approach that allowed for the sensitive evaluation of fine vessel blood flow using NIR-ICG AG. Our new classification system for evaluation of anastomotic perfusion was useful for predicting anastomotic leakage compared to conventional methods.
Conception and design of research: YM, H. Miyauchi, KS, H. Matsubara. Acquisition of data: YM, H. Miyauchi, GO, KN, KS. Analysis and interpretation of data: YM. Writing and editing of manuscript: YM, KH. Final approval of manuscript: YM, H. Miyauchi, GO, KH, KN, KS, H. Matsubara
The authors declare that they have no conflicts of financial and non-financial interest with the contents of this article.
Address correspondence to Dr. Yorihiko Muto.
Department of Frontier Surgery, Chiba University Graduate School of Medicine,
1-8-1, Inohana, Chuou-ku, Chiba 260-8670, Japan.
Phone: +81-43-222-7171. Fax: +81-43-226-2635.
E-mail:yorri1216apes@yahoo.co.jp
