




Chiba Medical J. 98E:9-18, 2022
doi:10.20776/S03035476-98E-2-P9
〔 Original Article 〕
Hiroaki Hosokawa1,2), Chenxu Huang3), Hiromichi Fujie3), Yuki Shiko4)
Shotaro Watanabe1,2), Manato Horii1), Masashi Shinohara1)
Yukio Mikami1), Kaoru Toguchi1), Seiji Kimura1,5), Ryuichiro Akagi1)
Satoshi Yamaguchi1,6), Seiji Ohtori1), and Takahisa Sasho1,2)
1) Department of Orthopedic Surgery, School of Medicine, Chiba University, Chiba 260-8670.
2) Center for Preventive Medicine, Musculoskeletal Disease and Pain, Chiba University, Chiba 260-8670.
3) Biomechanics Laboratory, Faculty of System Design, Tokyo Metropolitan University, Tokyo 192-0364.
4) Biostatistics Section, Clinical Research Center, Chiba University Hospital, Chiba 260-8677.
5) Department of Orthopedic Surgery, Center for Advanced Joint Function and Reconstructive Spine Surgery Graduate School of Medicine, Chiba University, Chiba 260-8670.
6) Graduate School of Global and Transdisciplinary Studies, Chiba University, Chiba 263-0022.
(Received November 18, 2021, Accepted December 7, 2021, Published April 10, 2022.)
【Objectives】Radial tears of the lateral meniscus are difficult to treat because the circumferential fibers that constitute the meniscal body are torn, and simple sutures intended to maintain both ends of the torn sites can easily slip and cut out. To overcome this, we developed a new suture construct to fix the radial tear in the meniscus. In this study, we examined the biomechanical properties of a new suture construct using a 6-degree-of-freedom (DOF) robotic system and a porcine knee.
【Methods】Five intact fresh frozen porcine knees and a 6-DOF robotic system was used in this study. First, we investigated whether a radial tear of the lateral meniscus would reduce the resultant force. Second, we investigated whether meniscal sutures would improve the resultant force. We also investigated the differences in the tibial shift and rotation.
【Results】The resultant force with a radial tear was significantly smaller than that with an intact meniscus, and the novel sutures and horizontal sutures improved the resultant force. The tibia shifted medially and posteriorly at 30° of knee flexion and medially at 45° of knee flexion with a radial tear below the 5 Nm valgus torque. Significant improvement was observed with the meniscus suture. Furthermore, the tibia rotated the valgus with a radial tear and improved with a meniscus suture under the 5 Nm valgus torque.
【Conclusions】Our new suture method may provide new insights into treatment of radially torn lateral meniscus with a minimum number of sutures.
Meniscus, Radial tear, Novel suture, Resultant force, Tibiofemoral relationship
It has become the gold standard to preserve meniscal tissue as much as possible upon surgical treatment for meniscal injury, as meniscectomy leads to secondary chondral lesions and osteoarthritic changes[1]. Thus proportion of meniscal repair increased compared to meniscectomy[2]. However, not all meniscal injuries can be repaired. The quality of meniscal tissue and vascularity are requisites for successful meniscal repair. Although both conditions are satisfactory, some types of meniscal injuries are still challenging for knee surgeons. Radial tears are representative of these cases. In this tear, the circumferential fibers that constitute the meniscal body are torn, and simple sutures intended to maintain both ends of the torn sites could easily slip and cut out [3-6]. To overcome the weakness of the repair construct, Nakata et al. invented tie-grip sutures, and James et al. reported a two-tunnel techinique[7,8]. Good clinical outcomes have been reported using the above techniques due to improved biomechanical strength[8-10]. However, a higher rate of chondral lesions was reported in the above-mentioned techniques [11]. We believe that the suture thread is one of the causes because it significantly interferes with the usual contact between the cartilage surface and the meniscal surface when the number of requisite sutures increases, as with tie-grip sutures, where a minimum of four to five throws of sutures are required. To overcome this, we developed a new suture construct to fix the radial tear in the meniscus. With this suture, we reduced the number of sutures to two. In this study, we examined the biomechanical properties of a new suture construct using a 6-degree-of-freedom (DOF) robotic system and a porcine knee.
Five intact fresh frozen porcine knees were used. The pigs were 6 months old and weighed approximately 105 kg. Specimens with osteoarthritis or ligamentous ruptures were excluded. The knees were cryopreserved and thawed at a low temperature for 24 h before use.
The tibias and femurs were cut to 100 mm in length from the joint line. All muscles were carefully removed from the knee, while the cruciate collateral ligaments and capsule were intact. The ends of the femur and tibia were fixed by molding acrylic resin (Ostron II; Momose Science Corp, Tokyo, Japan) into a cylindrical mold 130 mm high and 50 mm in diameter. The fibula was cut 50 mm in length from the proximal tibiofibular joint and fixed to the tibia using acrylic resin to maintain its anatomic position. Subsequently, the femoral and tibial cylinders were fixed to the clamps of the manipulator of the robotic simulator (Fig. 1).
Equipment
In this study, a 6-DOF robotic system (FRS-2015; Technology Service, Nagano, Japan) was utilized. The system consists of a velocity-control 6-DOF (three translational axes and three rotational axes) manipulator with a universal force/moment sensor (UFS) (Delta IP60; ATI Industrial Automation, USA) and a control computer (Windows 8; Dell, USA)[12-14]. The force/moment data from the UFS are input into a realtime controller (National Instruments, USA) using a multifunction DAQ (National Instruments, USA). Moreover, the control computer, real-time controller, and alternating-current (AC) servo system are connected by EtherNet and EtherCAT. The upper mechanism is linked to three translational-axis AC servomotors (X-axis and Y-axis are R2EA06020FXP00M; Sanyo Denki) and three rotational-axis AC servo actuators (U, V, and W axes are R2EA06020FXP00M; Sanyo Denki). AC servomotors power all actuators. Data on both the position and force/moment acting on the knee joint are acquired through the UFS, and the control computer operates the program in a graphical language programming environment (LabView 2013 real-time module; National Instruments, USA) to control the position and force/moment.
In this system, a knee joint coordinate system developed by Grood and Suntay was introduced and utilized. This system can manipulate the physiological three-dimensional (3D) motion of the knee joint by calculating and applying the 3D path to eliminate the force and moment on the knee joint, except for the operator’s intended direction. The clamp-to-clamp stiffness of the robotic system was 541-1027 Nm in translation and 262-355 Nm/rad in rotation. The frequency of data acquisition, kinematic and kinetic calculations, and motion of the actuators is 20 Hz. The tibial and femoral cylindrical molded ends were firmly connected to the manipulator’s upper and lower driving mechanisms, respectively, with custom-designed aluminum clamps.
Test protocols
Two experiments were conducted. First, we investigated whether a radial tear in the lateral meniscus would reduce the resultant force. Second, we investigated whether meniscal sutures would improve the resultant force. We also investigated the difference in tibial shift and rotation between the knees with the radially torn lateral meniscus and the sutured meniscus.
The knee flexion angle was defined as 20° of flexion with an extension moment of 1 Nm due to the intrinsic lag of the porcine knee. The knee joint was subjected to three flexion-extension tests between 20° and 130° under the following test conditions: (1) an axial load of 150 N and (2) a valgus moment of 5 Nm. The first and second tests were performed to eliminate creep in the knee joint, and the data from the third test were recorded. The lateral meniscus was performed under the following conditions: (1) an intact meniscus; (2) complete radial tear; (3) complete radial tear with a new suture technique; and (4) complete radial tear with horizontal suture. After we deeply flexed the knee joint so that the middle segment of the lateral meniscus could be visualized directly, radial sections were created in the middle segment of the lateral meniscus using scalpel #11 with no damage to the cartilage or soft tissues.
A new suture technique was done in three steps. First, we threw a single mattress suture in the posterior segment of the meniscus at a certain distance from the injured site, putting through most of the thread within the meniscal tissue. Next, another stitch was sutured distally to the mattress suture in the direction of the fibers of the meniscus, that is, perpendicular, and the thread was passed through the parenchyma and pulled out in front of the meniscus. Finally, we tie both ends of the anterior thread surface of the anterior horn of the meniscus (Fig. 2). We employed the standard double horizontal suture technique with parallel sutures as control (Fig. 3). All meniscus was repaired with No. 2-0 braided polyester and ultra-high-molecular-weight polyethylene suture (Fiberwire; Arthrex, Japan).
All cycles of the 3D path of the knee motion and the forces of three directions (fx, fy, fz) to the knee were recorded via UFS. After the test protocols were performed in each meniscal state, the lateral meniscus was removed. The simulator then reproduced all identical paths previously acquired under the four meniscal states, including the entire state and those with radial tears, while the forces (fx, fy’, fz) were also recorded. Based on the principle of superposition, the resultant force (F) was calculated and used for evaluation in the third cycle under 150 N axial load and 5 Nm valgus torque of:

The resultant force was defined as the meniscus carrying in response to a load applied to the knee joint and could be directly correlated with the meniscal function of the load distribution when axial compressive loads were applied to the knee. We recorded the resultant forces at 30°, 45°, 60°, 90°, and 120° under an axial load of 150 N and valgus torque of 5 Nm. The values of axial load and valgus torque were determined based on the previous report [15]. We also considered for axial load of 250N, but it was decided not to use because it was thought to pose a risk of failure of the robot system in preliminary experiments.
Additionally, the 3D position of the tibial relative to the femur under 150 N axial load and 5 Nm valgus torque was also evaluated in the third cycle in each meniscal state. The tibial shift was measured as the difference between the tibial position in the intact meniscus and the tibial position in each state of the meniscus in the medial-lateral and anterior-posterior directions. The tibial rotation was measured as the difference between the position of the tibia in the intact meniscus and the position of the tibia in each state of the meniscus in the internal and external rotation directions. We recorded the tibial shift and rotation at 30°, 45°, 60°, 90°, and 120° under an axial load of 150 N and valgus torque of 5 Nm.
Statistical analysis
We used the linear mixed-effects model to compare the resultant force and tibial shift between the groups at each knee flexion angle. We designated subjects as random effects for the mixed model, while the flexion angle and group (including their interaction terms) were treated as fixed effects. Post hoc tests for multiple comparisons were performed using the Bonferroni’s significant difference test, and statistical significance was set at p < 0.05. All statistical analyses were performed using the SAS statistical software package (version 9.4; SAS Institute, Cary, NC, USA).
Fig. 1 6-DOF robotic system. The femur is fixed to the upper mechanism, while the tibia is fixed to the lower mechanism via a universal force/moment sensor.
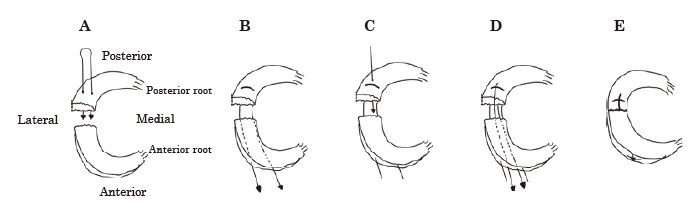
Fig. 2 Procedure for a novel suture method. (A) First, we throw a single mattress suture in the posterior segment of the meniscus at a certain distance from the injured site. (B) Next, we put through most of the thread within the meniscal tissue. (C) Third, another stitch is sutured distally to the mattress suture in the direction of the fibers of the meniscus. (D) The thread is passed through the parenchyma and pulled out in front of the meniscus. (E) Finally, we tie both ends of the anterior thread surface of the anterior horn of the meniscus.
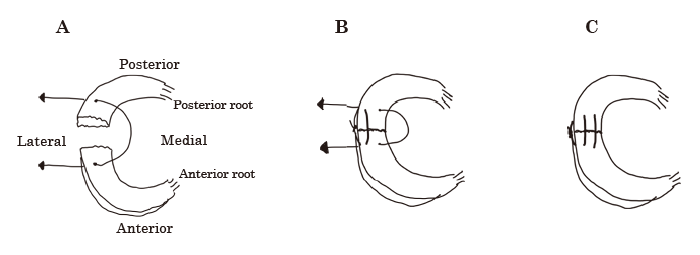
Fig. 3 Procedure for a horizontal suture method. (A) First, we applied thread horizontally to both ends of the injured area. (B) Next, we applied the suture parallel to the first thread. (C) Finally, we tied the end of the suture.
Resultant force
The resultant force with a radial tear was significantly lower than the intact meniscus at 30°-120° of knee flexion under an axial load of 150 N (Fig. 4A). Similarly, under the 5 Nm valgus torque, the resultant force with a radial tear was significantly lower at 30°-120° of knee flexion (Fig. 4B).
Next, we examined whether meniscus sutures would improve the resultant force. The resultant force with the novel suture was significantly higher than the lateral meniscus with radial tear at 45° of knee flexion under an axial load of 150 N and 30°-60° under 5 Nm valgus torque (Fig. 5A). The resultant force with horizontal suture was significantly higher than that with a radial tear and was significantly lower only at 60° of knee flexion under 5 Nm valgus torque (Fig. 5B).
Tibiofemoral relationship
The tibia shifted medially and posteriorly at 30° of knee flexion and 45° of knee flexion with a radial tear under 5 Nm valgus torque. Significant improvement was observed with the meniscus suture (Figs. 6B, 7B). Moreover, the tibia rotated the valgus with a radial tear and improved with meniscus suture at 30°-120° of knee flexion under 5 Nm valgus torque (Fig. 8B). There was no significant difference in internal or external rotation (Fig. 9B). The tibia did not shift or rotate significantly under an axial load of 150 N (Figs. 5-8A).
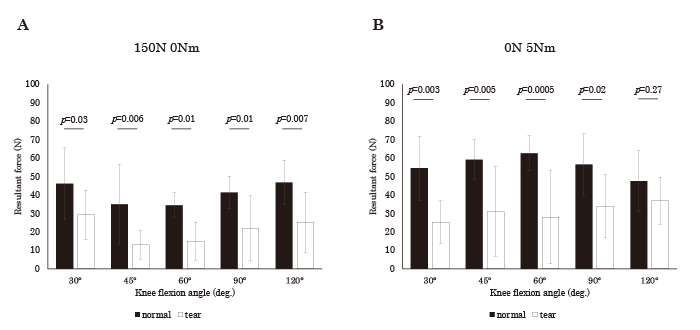
Fig. 4 The resultant force of an intact meniscus and a complete radial tear under (A) 150 N axial load and (B) 5 Nm valgus torque. Under the two test conditions, the resultant force is significantly reduced by the radial tear at all angles.
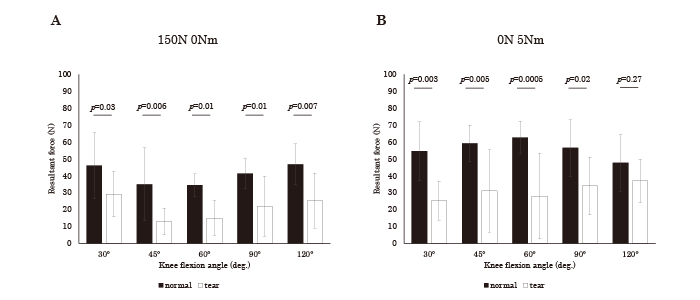
Fig. 5 The resultant force of an intact meniscus and a complete radial tear under (A) 150 N axial load and (B) 5 Nm valgus torque. (A) Under the 150 N axial load, the resultant force increases significantly in the novel suture compared with the radial tear at 45° of knee joint flexion. Although there are no significant differences in other angles, the novel suture and horizontal suture have higher resultant force than the radial tear. (B) Under the 5 Nm valgus torque, the resultant force of the novel suture is significantly higher than radial tear at 30°-60° of the knee joint flexion. At 60° of knee joint flexion, horizontal tear also significantly improved the resultant force compared to the radial tear. Although there were no significant differences in other angles, the novel suture and horizontal suture had higher resultant force than the radial tear.
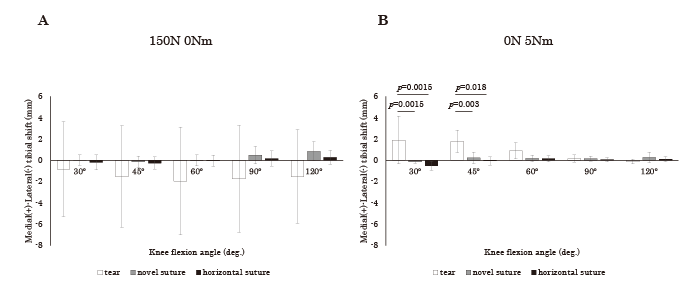
Fig. 6 The medial and lateral tibial shift under (A) 150 N axial load and (B) 5 Nm valgus torque. (A) Under the 150 N axial load, the tibia shifted laterally due to the radial tear, but there was no significant difference. (B) Under the 5 Nm valgus torque, the tibia was significantly shifted medially by a radial tear at 30°-45° of knee joint flexion, which was improved by both suture methods.
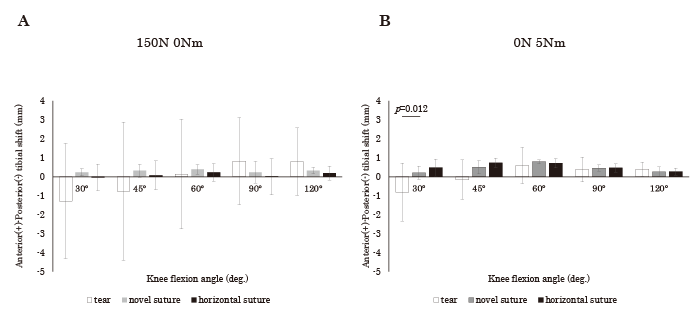
Fig. 7 Anterior and posterior tibial shift under (A) 150 N axial load, and (B) 5 Nm valgus torque. (A) Under the 150 N axial load, there are no significant differences in the shift of the tibia in each group. (B) Under the 5 Nm valgus torque, the tibia shifted posteriorly by a radial tear at 30° of knee joint flexion and improved significantly by the novel suture, but there is no significant difference at other knee joint flexion angles.
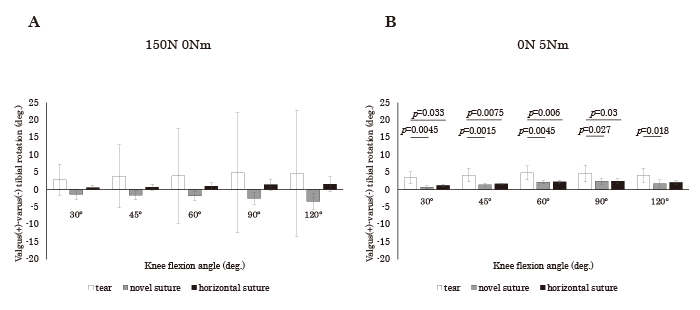
Fig. 8 Valgus and varus tibial rotation under (A) 150 N axial load and (B) 5 Nm valgus torque. (A) Under the 150 N axial load, there are no significant differences between the three groups. (B) Under the 5 Nm valgus torque, the radial tear's tibial rotation is observed at all angles, but a significant improvement is observed in the novel suture and horizontal suture.
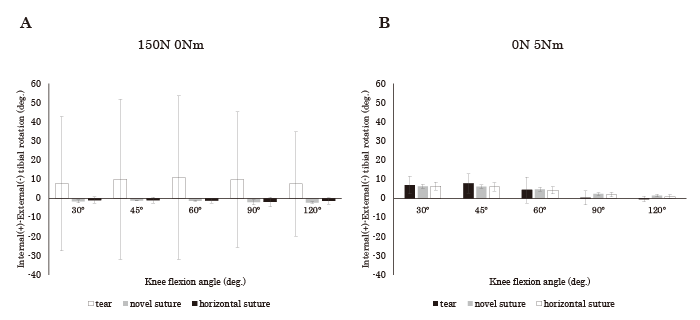
Fig. 9 Internal and external tibial rotation under (A) 150 N axial load and (B) 5 Nm valgus torque. There are no differences between the groups under the two test conditions.
In the present study, a newly designed suture construct for the repair of a radial meniscal tear was biomechanically studied using the whole knee joint of the porcine and 6-DOF robotic system. As a result, the construct could recover the meniscal function better than simple horizontal sutures in some parameters.
This is the first report that showed recovery of meniscal function after meniscal repair under mimicking in vivo circumstances in which significant knee joint structures were kept undisturbed using the 6-DOF robotic system.
Previous biomechanical studies dealing with meniscus injury and repair could be classified into three.
First, ex vivo studies in which menisci were removed from cadavers or animal knees. They were then placed on a uniaxial material testing machine to measure the gap created at the injured site after cyclic loading and analyze the failure mode[4,16].
Second, studies that mimicked in vivo circumstances in which whole knee joints were used. In this type of studies, a pressure sensor was inserted between the meniscus and the tibial cartilage after creating and repairing meniscal injuries. Although researchers tried to reproduce intra-joint circumstances, some procedures in knee joints were inevitable, such as osteotomy of the femoral condyle[17]or cutting the lateral collateral ligament[18]. In addition, the thickness of the pressure sensor may disturb the reproduction of intra-joint circumstances.
Third, studies that conducted using intact knee joints other than the menisci. As far as the literature search could reach, the system used in the present study was the only way to achieve this. However, prior to the present study, only the effect of meniscal injury on the resultant force was examined. Radial tears of the lateral menisci[15], longitudinal tears of the medial menisci [19], and partial meniscectomy of the medial meniscus [20]have been studied. The present study is the first to analyze the effect of meniscal repair under reproduction in the in vivo knee joint.
We believe that the third type of study should be performed first to test the efficacy of the suture construct. We detected different biomechanical properties of the two types of constructs. Although the two constructs showed an improved resultant force or tibial shift simultaneously, the novel sutures could achieve different resultant forces at 30°, 45°, and 60° of knee flexion.
Compared with other types of meniscal injuries, radial tears are challenging to repair. Therefore, several suturing techniques have been proposed, some of which have been used in actual surgeries. Even with these techniques, second-look arthroscopy showed a relatively low healing rate. Tsuji et al. reported a failure rate of 39% (7/18) after tie-grip suture using the standard gold method at present[9]. Furthermore, a higher rate of chondral lesions was reported after tiegrip suture[11]. The inevitable existence of four to five suture threads on the meniscal surface might cause chondral lesions. Therefore, there appears to be a need for further improvements in repair techniques. In the present study, we attempted to reduce the suture threads to two and compared them with the conventional suture method (horizontal suture) with the same number of threads. Although the new technique showed a mostly comparable results to the conventional suture method, it showed statistically bigger resultant force at 30° and 45° of knee flexion whereas conventional method did not. Still, we did not think that the new technique was sufficient for clinical use. The resultant force at 90° and 120° of knee flexion should be improved.
Further modification might overcome these shortcomings, but a postoperative rehabilitation program might be helpful. A restricted flexion angle of the knee joint for a certain amount of time until healing might help achieve good meniscal function. The possible role of the 6-DOF robotic system in determining rehabilitation programs was also elicited.
There are some limitations to this study. First, the use of porcine knee joints instead of human knees. Porcine is the standard animal model for biomechanical studies of menisci and can provide menisci with homogenous properties, but its morphological and biomechanical properties differ from those of human knee joints. Second, we did not compare the new technique with the tie-grip suture or the two-tunnel technique, but our goal was to achieve a better suture construct with a minimum number of sutures. We may have to deal with other sutures in the future. Third, we did not evaluate the difference in cartilage damage due to suture method. Further investigation that dealt with cyclic loading under in vivo circumstances should be performed.
In conclusion, our new suture method may provide new insights into treatment of radially torn lateral meniscus with a minimum number of sutures.
HH and TS contributed to the development of anovel suture method. HH, TS, and HF contributed to the conception and design of the study. HH and SK performed biomechanical tests. HH analyzed the data obtained from the experiment. YS contributed to the statistical analysis. HH wrote the first draft of the manuscript, and all authors commented on the subsequent versions. SK, RA, SY, SO, and TS provided constructive comments and revised the manuscript. All authors read and approved the final manuscript.
No specific funding was used for this study.
S.O. is a member of the Editorial Board of the Chiba Medical Journal.
This study does not contain any experiments with live animals because all knee specimens were obtained from edible pigs from the local butcher. Therefore, ethical approval for animal research was not required in this study.
All data generated or analyzed during this study are included in this published article.
The authors thank Yasuraku Shibata for the guidance in the operation of 6-DOF robotic system and the cooperation in the preliminary experiments.
Address correspondence to Dr. Hiroaki Hosokawa.
Department of Orthopedic Surgery, Graduate School of Medicine,
Chiba University, 1-8-1 Inohana, Chuou-Ku, Chiba 260-8670, Japan.
Phone: +80-43-226-2117.
E-mail:brotherf00t.hiro.hoso@gmail.com
