




Chiba Medical J. 88E:59~64,2012
doi:10.20776/S03035476-88E-6-P59
[Original Paper]
Shihoko Namba1,3), Ichiro Shimoyama2), Takashi Kiguchi3) and
Yoshihito Ujike4)
1) Department of Cognitive Behavioral Physiology, Graduate School of Medical and Pharmaceutical Sciences, Chiba University, Chiba 260-8670.
2) Human Neurophysiology, Frontier Medical Engineering, Chiba University, Chiba 263-8522.
3) Department of Nursing, Okayama University Hospital, Okayama 700-8558.
4) Emergency and Critical Care Medicine, Graduate School of Medicine, Okayama University, Okayama 700-8558.
(Received January 20, 2012, Accepted November 8, 2012)
Patients in intensive care units(ICU) are exposed to stress because of invasive medical treatments, serious diseases, and the uncomfortable environment. The possibility of sleep disorders is high under these conditions. Many Japanese nurses perform foot baths to bring patients comfort.
A single group crossover design was used to examine the effects of foot baths on the sleep outcome in six ICU patients. This study examined the characteristics of these ICU patients. Polysomnograms were recorded for two nights; a foot bath night and non-foot bath night.
At least one non-foot bath day was provided between foot bath days.
The patients were randomly assigned to receive a foot bath at 40°C for 10 min before sleep onset on one of the two nights. No significant difference was found in the total time for each sleep stage between the non-foot bath and foot bath nights; however, the total time was found to be significantly different among the four sleep stages on foot bath nights by an analysis of variance(P<0.01).
No difference was noted in sleep stages III+IV regardless of whether foot baths were given. However, the patients claimed that they slept well the night after receiving a foot bath. Therefore, the polysomnographic results and subjective assessments did not match.
foot bath, sleep, polysomnograms, ICU
Stress is a problem for patients in intensive care units(ICU)[1]. Stress impairs the patients’ sleep, resulting in frequent medication with narcotics. Various monitors and tubes, noise from respirators and other machines, and frequent examinations all cause stress in the patients[2-6]. Sleep deprivation impinges on recovery. Insomnia compromises the ability to resist infection, exacerbates neurological problems such as delirium, and causes respiratory problems because it weakens upper airway muscles, thus prolonging the duration of ventilation, ICU stay, and recovery after extubation[7,8].
Therefore, high-quality sleep is important to secure the patients’ health. One technique used for inpatients in Japan to promote sleep is bathing of the feet. Foot bathing is routinely performed by nurses in critical care units. The main purpose of foot bathing is to keep the feet clean and to relieve stress. The propensity of foot warming to improve sleep quality changes with age and helps attenuate age-related insomnia[9]. Recently, foot bathing has been reported to decrease the heart rate and respiratory rate and to shorten the time to sleep onset[10].
The relationship between foot bathing and sleep has been investigated in healthy people[11], but few studies have examined this relationship in the context of critical medical care. This study examined the relationship between foot bathing and sleep in ICU patients.
Participants
The patient characteristics are summarized in Table 1(Table 1). Three females and three males, with a mean age of 65 years, participated in this study. Five patients were hospitalized in private rooms, and one in a semi-private room. The pathogeneses included trauma, hemorrhagic shock and respiratory disease. Two patients had been prescribed sedatives which affected sleep directly. Three patients had been prescribed sleep medications.
Patients were eligible for the study only if they had been admitted to a high care unit or ICU and had received permission from their attending physician. The patients were divided into two groups and received foot baths on one of two designated days. The bathing room was the same for both groups. All patients provided their informed consent. The following patients were excluded:head injury/neurotrauma patients, burn patients, and comatose patients.
Table 1
Clinical features of the subjects
Experimental procedure
In this crossover design study, polysomnograms (PSG) were recorded for six ICU patients from October 2010 to October 2011. The study protocol was approved by the research ethics board of Okayama University Hospital.
A polysomnograph(Alice PDx®, Philips Respironics, Murrysville, PA, USA) was used to record the total sleep time(TST), duration of rapid eye movement(REM), duration of sleep stages I, II, and III+IV, arousal and awake times, and oxygen saturation(SpO2). The polysomnograph is a miniature device that utilizes standard electroencephalography, electromyography, oximetry, and position sensors with post-study technician scoring. The recording order was assigned using a random number table. Thus, the PSG was recorded during the night either after a foot bath or without a foot bath. The patients in the two groups had alternating footbath days.
A schedule was established for the foot bath and non-foot bath days. PSG was performed from 21:00 hrs to 06:00 hrs on both days. The patients were situated in a semi-Fowler’s position, and received foot baths for 10 min. Basins were filled with warm water(40°C) up to the ankle. Each foot bath was followed by bed rest.
Subjective evaluations with regard to sleep were also performed. Patients who could communicate well were asked about the quality of sleep on the foot bath and non-foot bath nights.
If patients complained of pain or discomfort, foot bathing was stopped immediately. Changes in circulation were noted. At a minimum, an interval will be set on the 1st or more.
The schedule of foot bath days and non-foot bath days was discontinued. At the very least, an interval of one or more non-foot bath days was scheduled between the foot bath days.
Data analysis
All data were represented as the means ± standard deviation(SD) or as percentages. To identify differences between foot bath and non-foot bath nights, a paired sample t-test was used. A repeated measures two-factor analysis of variance(ANOVA) was used to examine the differences among the values for the duration of REM and stages I, II, and III+IV sleep for foot bath and non-foot bath nights. When significant interactions were detected, Bonferroni multiple comparisons were performed.
Data were analyzed using the SPSS® version 16.0 software program(SPSS Inc., Chicago, IL, USA)P values <0.05 were considered to be statistically significant.
Figure 1(Fig. 1) shows a sample PSG from one subject. The characteristics of this patient are summarized in Table 1(Table 1). The results for the TST are shown in Figure 2(Fig. 2), and the ratios for each sleep stage are shown in Figure 3(Fig. 3). Significant differences were observed among the four stages in the foot bath and non-foot bath groups, as shown in Figure 4(Fig. 4)( P<0.01, ANOVA). Stage III+IV did not appear in the non-foot bath group at all, but a short duration of this stage appeared in the foot bath group.
The frequency of arousal or waking per night was 125 times(SD: ±72.9) on non-foot bath nights and 143.7 times(SD: ±49.5) on foot bath nights(Fig. 6). No significant difference was observed between these frequencies. Figure 7(Fig. 7) shows the SpO2 levels. The mean was 96.5%(SD: ±0.2) on non-foot bath nights and 95.8%(SD: ±0.3) on foot bath nights. No significant difference was noted between the nights.
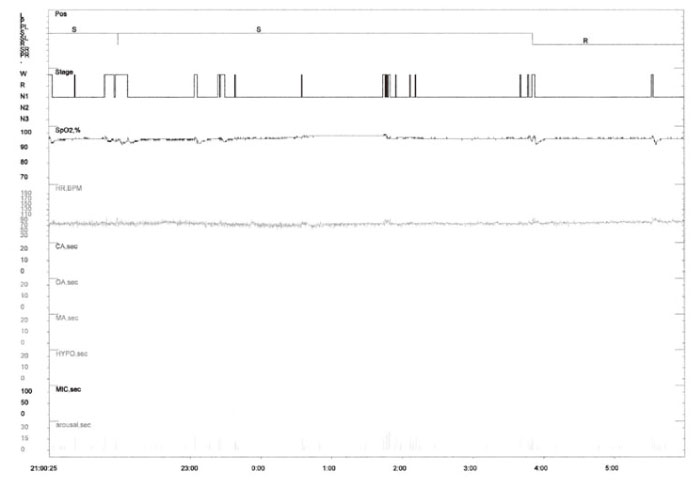
Fig.1
Actual data notation on polysomnography
Fig.2
The total sleep time for the control and foot bath groups.
The total sleep time showed no significant difference between the groups.
Fig.3
The sleep efficiency of the control and foot bath groups.
The sleep efficiency was not significantly different between the two groups.
Fig.4
The times spent in different sleep stages(min) for the control and foot bath groups.
The total time spent in the sleep stages was not significantly different between the two groups, but the total time spent asleep was significantly different among the two groups(P<0.01, ANOVA).
Fig.5
The sleep stage(%) for the control and foot bath groups.
The total time spent in the different sleep stages was not significantly different between the groups, but the total time spent asleep was significantly different in the control and foot bath groups(P<0.01, ANOVA).
Fig.6
The frequency of arousal and awakening for the control and foot bath groups.
The ordinate represents the number of times the patient awoke in one night.
No significant difference was observed in the frequency of arousal and awakening in the control and foot bath groups.
Fig.7
The oxygen saturation in the control and foot bath groups.
The oxygen saturation was not significantly different between the two groups.
The mean TST for non-foot bath nights was 331.4 (SD: ±47.1) and that for the night after the foot bath was 318.5(SD: ±29.6). No significant differences were found in the TST between the nights(P=0.665; Fig. 2)(Fig. 2). Sleep efficiency was defined as the total sleep time/time in bed × 100. The mean sleep efficiency for non-foot bath nights was 61.3( SD: ±8.9), while the mean sleep efficiency for foot bath nights was 58.1 (SD: ±5.3). No significant differences were observed in the sleep efficiency between non-foot bath and foot bath nights(P=0.543; Fig. 3)(Fig. 3).
The total time for REM and sleep stages I, II, and III+IV was also studied. The mean REM time was 44 min(SD: ±11) for the non-foot bath nights and 50.3 min(SD: ±13.5) for the foot bath nights. The mean time spent in stage I was 150.2 min(SD: ±73.5) for non-foot bath nights and 124.4 min(SD: ±50.3) for foot bath nights. The mean time spent in stage II was 44 min(SD: ±11) for non-foot bath nights and 50.3 min (SD: ±13.5) for foot bath nights. The mean time spent in stage III+IV was zero for non-foot bath nights and 3.7 min( SD: ±2.4) for foot bath nights. No significant differences were observed between the sleep stages for non-foot bath and foot bath nights(Table 2).
All four patients who could communicate without difficulty reported“sleeping well” on foot bath nights.
Table 2
The sleep periods and time spent in sleep stages for the control and foot bath groups
No differences in the PSG were noted between the non-foot bath and foot bath nights. The TST was not longer on the foot bath than on non-foot bath nights. REM sleep was increased on the foot bath nights. No significant differences were noted among the sleep stages. However, the patients subjectively reported sleeping well after receiving a foot bath. Psychological factors may thus be responsible for the differences in PSG results compared with subjective reports.
A previous study reported decreased wakefulness in the non-REM period on foot bath nights[12]. In their study, the duration of foot bathing was 40 min. In our study, the foot bath time was limited to 10 min out of consideration of the patients’ situations. Patients in the ICU are easily fatigued and sometimes have difficulty holding the same position for longer than a few minutes. No differences were recorded by the PSG between the TSTs for the non-foot bath and foot bath nights in our study.
Insomnia is a common complaint in ICU patients and is caused by a variety of factors. One questionnaire study reported that a patient’s sleep quality in the ICU was significantly worse than their baseline sleep at home. Environmental noise was an important contributor to sleep disruptions in ICU patients[13].
Many causes of insomnia have been reported, including age, psychological problems, the influence of medication(s), and environmental factors[13,14]. Most ICU patients are subject to at least one of these risk factors. Parthasarathy and Tobin reported that ICU patients who have difficulty falling asleep spend less time in REM sleep, wake more frequently than normal, and are awakened from sleep by noise, anxiety, pain, frequent treatments and nursing care interventions, as well as noise from monitors[15]. However, only a few studies have so far examined sleep in ICU patients using PSG. In addition, how each of these factors affects sleep is unknown. One of the reasons could be the difficulty in measuring sleep. PSG is the gold standard method for measuring sleep, particularly in the evaluation of sleep stages. However, sensors can become a nuisance to the subjects. Therefore, a simple commercial PSG consisting of eight sensors attached to the face and a recording unit was used in this study.
Normally, people fall asleep within approximately 20 min and enter successively deeper stages of non-REM sleep, with REM periods occurring about 90 min after sleep onset and‘90-120’ min thereafter. Typically, deeper non-REM sleep is seen in the first half of the sleep period, and more REM sleep occurs in the second half[16]. In general, Sleep efficiency greater than 80% is regarded as normal. Sleep efficiency less than 80% is considered insomnia. In our study, the sleep efficiency was 61.3%, and no time was spent in sleep stages III+IV. This result suggests that ICU patients found it difficult to sleep comfortably. In a previous study on elderly people(mean age, 67 years), the average sleep efficiency was 84.8% and the time spent in sleep stage III+IV was 3.4%[12]. The quality of sleep in the elderly was inferior to that in younger people. The mean age was similar(65 years), but the sleep quality was inferior, in our study. Frequent pharyngeal aspiration and postural care every two hours may make patients irritable and prevent them from entering sleep stages III and IV when they are in the ICU.
All patients had an underlying disease in our study. One patient had a history of mental disease, and some were suspected of having sleep apnea. In addition, a possible association of sleeplessness with medication use cannot be ignored. Various medications affect sleep quality, such as vasopressors, inotropes, gastric protectors, antibiotics, anticonvulsants, and steroids. The administration of dopamine, epinephrine, and norepinephrine has been shown to decrease the slowwave and REM sleep through adrenergic receptors[16].Medications were discontinued before PSG recording in our study.
In conclusion, PSG showed no differences in the sleep time between non-foot bath and foot bath nights, but patients reported sleeping well after receiving a foot bath. Thus, foot baths may relieve stress in ICU patients.
This work was supported by nurses in the high care unit/intensive care unit of Okayama University Hospital. We thank the staff members of Philips Respironics and Mizusawa for their invaluable help during the analyses.
Abbreviations: ICU; Intensive care unit, PSG; Polysomnograms, REM: Rapid eye movement
Address correspondence to Dr. Shihoko Namba.
Human Neurophysiology, Frontier Medical Engineering, Chiba University, 1-33, Yayoi-cho, Inage-ku, Chiba 263-8522, Japan
Phone: +81-43-290-3118. Fax: +81-43-290-3118.
E-mail: namba-s1@cc.okayama-u.ac.jp
