




Chiba Medical J. 89E:15~19,2013
doi:10.20776/S03035476-89E-3-P15
[Case Report]
Yuya Ogawa, Kazuhide Inage, Sumihisa Orita, Kazuyo Yamauchi
Yasuchika Aoki, Tetsuhiro Ishikawa, Masayuki Miyagi, Hiroto Kamoda
Miyako Suzuki, Gou Kubota, Yoshihiro Sakuma, Yasuhiro Oikawa
Takeshi Sainoh, Jun Sato, Junichi Nakamura, Masashi Takaso
Gen Inoue, Tomoaki Toyone, Kazuhisa Takahashi and Seiji Ohtori
Department of Orthopedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
(Received February 6, 2013, Accepted March 22, 2013)
Purpose: Spinal kyphosis in elderly people sometimes causes severe low back pain. Surgical methods such as pedicle subtraction osteotomy (PSO) are useful for correcting the deformity. However, complications during surgery, the occurrence of pseudarthrosis and need for revision surgery are problems associated with the PSO procedure. The purpose of the current study was to present a case of revision surgery for pseudarthrosis and implant failure after PSO in a patient with adult kyphosis.
Methods: A 68-year-old woman previously underwent transforaminal lumbar interbody fusion because of lumbar spinal stenosis. After the surgery, she underwent lumbar PSO because of adjacent junctional kyphosis. Six months after her second surgery, pseudarthrosis, and breakage of instrumentation was found on X-ray examination.
Results: We performed combined posterior and anterior fusion surgery. Dual rods were used in posterior surgery, and 2 mesh cages, autograft from a rib, and a 2 rod-plate system were used in anterior surgery. The patient became symptom-free after surgery. Bony fusion was observed 6 months after surgery.
Conclusions: We performed combined posterior and anterior fusion surgery for a patient who showed symptomatic pseudarthrosis after PSO surgery. We concluded that the combined surgery was effective.
Revision surgery, pseudarthrosis, implant failure, pedicle subtraction osteotomy, adult kyphosis
Spinal kyphosis in elderly people sometimes causes serious problems. It occurs as a consequence of the loss of the physiological lordotic curve because of senile kyphosis, which is attributed to osteoporosis, disk degeneration, and impairment of back muscles.[1,2] The postural abnormality associated with kyphosis can not only cause chronic low back pain, but, in later stages, can also disturb standing and gait by affecting balance.[3] There have been multiple surgical procedures described for the treatment of spinal kyphotic deformity. These have included Smith-Petersen osteotomy (SPO), pedicle subtraction osteotomy (PSO), and vertebral column resection (VCR) procedures. The technique used to correct spinal kyphotic deformity depends on factors such as the severity of the deformity, the flexibility of the deformity, and whether the kyphosis is more of a rounded, long sweeping kyphosis or a short, angular one. An SPO can provide about 10° of correction, whereas a PSO can provide about 35° of correction, and a VCR can provide 40° degree of correction or more[4,5]
Suk et al. have reviewed the treatment of 70 spinal deformity patients by posterior VCR. Mean operation time was over 4 hours with average blood loss of 2333 mL, and complications were encountered in 34% patients.[6] Kim et al. have reported the treatment of 35 consecutive patients with sagittal imbalance using lumbar PSO. However, there was an occurrence of pseudarthrosis and need for revision surgery in 8 of 35 (23%) patients.[7] In this regard, we need to be aware of the high complication rate and revision surgery because of complication after these surgical methods. The purpose of the current study was to present a case of revision surgery for pseudarthrosis and implant failure after PSO in a patient with adult kyphosis.
Patient
Written, signed consent was received from the patient before treatment.
In July 2011, a 68-year-old woman presented with a 1-year history of low back pain and bilateral sciatica with complaints of pain in her buttocks and the lateral aspects of her legs. There was motor weakness of hamstrings, and the tibialis anterior muscle of her right leg. Sensory examination confirmed hypalgesia in the lateral aspect of her upper and lower leg corresponding to the L3, L4, and L5 dermatomes on both sides. Deep tendon reflex was normal in both legs. There was apparent urinary disturbance. Bilateral straight leg raising test results were negative.
In her history, she underwent transforaminal lumbar interbody fusion at L3-L4 and L4-L5 because of lumbar spinal stenosis in 2003. She underwent PSO at L2 level because of adjacent junctional kyphosis in 2010. Six months after her second surgery, breakage of instrumentation was found on X-ray examination.
X-ray examination showed pseudarthrosis of L2, L1 retrospondylolisthesis, and breakage of bilateral rods (Fig.1).. Myelograms showed instability and severe L1 retrospondylolisthesis between flexion and extension positions (Fig.2).. As conservative treatment was not effective, surgery was planned. We performed combined posterior and anterior fusion surgery. At first, rods were removed, and dual rods were used in posterior surgery (total 4 rods were used during surgery) (Fig.3).. Next, 2 mesh cages, autograft from a rib, and a 2 rodplate system were used in anterior surgery. The patient became symptom-free after surgery. At 6 months after surgery, bone fusion was observed, and there was no breakage of instrumentation (Fig.4)..
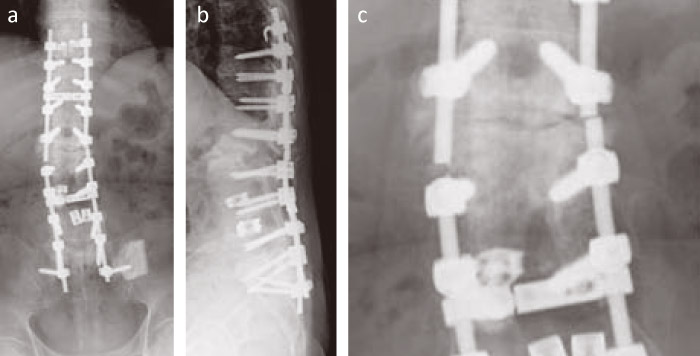
Fig.1
X-ray film images from a 68-year-old woman 6 months after PSO surgery. Anterior-posterior view (a), lateral view (b), and magnification of the area of rod breakage (c).
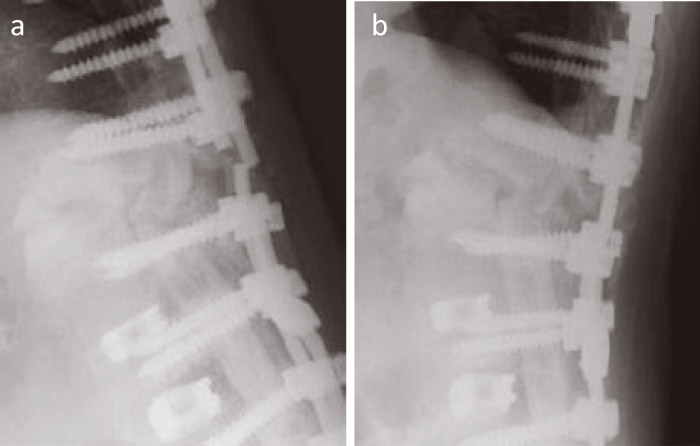
Fig.2
Lateral view of myelogram. Flexion position (a) and extension position (b). There was apparent instability at pseudarthrosis.

Fig.3
Photograph showing posterior view during surgery. New long rods and additional satellite rods were inserted at posterior surgery.
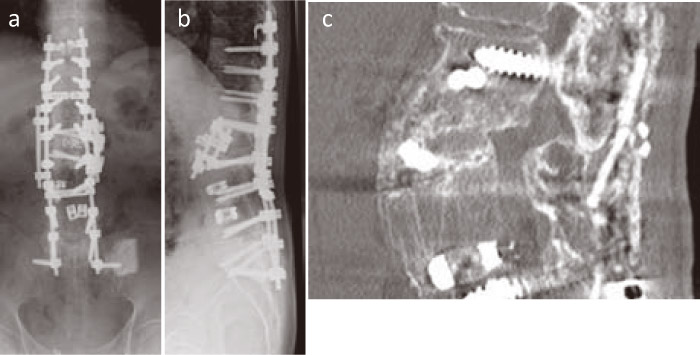
Fig.4
X-ray films and three-dimensional CT 6 months after surgery. Anterior-posterior view (a), lateral view (b), and sagittal view of CT imaging (c). Complete bony fusion was observed 6 months after surgery.
In the current report, we present a case of revision surgery for pseudarthrosis and implant failure after PSO in a patient with adult kyphosis. We selected a combination of anterior and posterior fusion surgery for the patient. Bony union was observed within 6 months after surgery, and we concluded that this combination was effective for unstable pseudarthrosis and implant failure after PSO in patients with adult kyphosis.
As mentioned in the introduction, PSO is effective for correction of kyphosis. However, high rates of complications have been reported. The Scoliosis Research Society Morbidity and Mortality Committee have reported the short-term complication rate in patients undergoing treatment of thoracolumbar fixed sagittal plane deformity.[8] Five hundred and seventyeight cases including PSO cases were analyzed. The rate of complication was 29.4% in all patients and there were deaths (0.5%). The most common complications were durotomy (5.9%), wound infection (3.8%), new neurologic deficit (3.8%), implant failure (1.7%), wound hematoma (1.6%), epidural hematoma (1.4%), and pulmonary embolism (1.0%). Procedures including an osteotomy had a higher complication rate (34.8%) than cases not including an osteotomy.[8] A retrospective review of prospectively collected data from 6 centers in France has been reported[9] . A total of 306 primary lumbar adult or degenerative scoliosis patients older than 50 years undergoing PSO surgery between 2002 and 2007 were included. The overall rate of complications was 39%. Pseudarthrosis or lateinstrumentation failure with rod breakage was seen in 19.3%, and these patients underwent revision surgery for mechanical complications.[9] In this regard, we need to take these complications into consideration when performing PSO surgery.
On the other hand, some authors have reported difficulties in revision surgery for pseudarthrosis. Lauerman et al. have reported that 40 patients underwent 47 procedures for repair of a lumbar pseudarthrosis, and 43 procedures in 36 patients with a minimum followup of 2 years were reviewed.[10] Solid fusion was achieved in only 49% of cases.[10] In another report, 63 first, second, or third-time repairs of one or more pseudarthroses were required in 51 patients who had an arthrodesis for idiopathic scoliosis.[11] Failure of the implant was identified before 27% of the 63 procedures.[11] Symptomatic pseudarthrosis are most common in the thoracolumbar and lumbosacral regions, and revision surgery for symptomatic pseudarthrosis is characterized by a high rate of recurrent pseudarthrosis and clinical failure.[12]
In the current study, we used both anterior and posterior surgery for revision after pseudarthrosis and implant failure after PSO. Generally, the thoracic spine is more stable compared with the thoracolumbar and lumbar spine. Thus, Berven et al. have reviewed the long-term clinical and radiographic results of posterioronly surgery for the treatment of pseudarthrosis in the thoracic spine.[13] Only single-stage posterior revision surgery with extension osteotomies through the regions of pseudarthrosis coupled with rigid internal fixation and autogenous bone grafting is an effective technique for treatment of pseudarthrosis of the thoracic spine.[13] By contrast, reviews of repeated fusion for failed surgery in the lumbar spine show a 50% to 65% fusion rate and a clinical failure rate as high as 40% to 70% in patients with symptomatic lumbar pseudarthrosis.[10,14] Most pseudarthrosis repair techniques reported in the literature concentrate on posterior fusion with no instrumentation or posterior fusion with instrumentation.[10,14] On the other hand, Albet et al. attempted to determine the radiographic and functional results of a combined anterior-posterior surgical procedure to manage symptomatic pseudarthrosis of the lumbosacral spine.[15] The radiologic and clinical results are superior to those previously reported for the use of posterior instrumented or noninstrumented pseudarthrosis repairs.[15]
Biomechanical study revealed the importance of the anterior portion of the spine such as intervertebral discs for spinal stability. The role of degenerated intervertebral discs in degenerative spinal instability has previously been clarified by means of biomechanical cadaver studies.[16,17] In one study on flexion-extension and axial rotation, the flexibility parameters increased with disc degeneration.[17] Another cadaver study revealed that axial rotational motion was more affected by disc degeneration rather than posterior facet joints, and segmental motion increased with increasing severity of disc degeneration.[16] For these reasons, we selected anterior and posterior surgery for revision of unstable pseudarthrosis and implant failure after PSO in the current study.
The current study is limited to this single case report. Nevertheless, further studies are warranted into the efficacy of anterior and posterior surgery for revision after pseudarthrosis and implant failure after PSO.
In conclusion, we performed combined posterior and anterior fusion surgery for a patient who showed symptomatic pseudarthrosis after PSO surgery. The patient became symptom-free after surgery, and solid bony fusion was achieved. This combined surgery was effective for our patient’s unstable spine.
None.
The authors did not receive any financial funding for data collection, analysis, or writing of the manuscript.
The authors did not receive and will not receive any benefits or funding from any commercial party related directly or indirectly to the subject of this article.
Address correspondence to Dr. Seiji Ohtori.
Department of Orthopedic Surgery, Graduate School of Medicine, Chiba University, 1-8-1 Inohana, Chuo-ku, Chiba 260-8670, Japan.
Tel.+81-43-226-2117. Fax. +81-43-226-2116.
E-mail: sohtori@faculty.chiba-u.jp
