




Chiba Medical J. 90E:31~35,2014
doi:10.20776/S03035476-90E-5-P31
[Original Paper]
Yoshimasa Ono, Seiji Ohtori, Sumihisa Orita, Kazuyo Yamauchi
Yasuchika Aoki, Masayuki Miyagi, Miyako Suzuki, Gou Kubota
Yoshihiro Sakuma, Yasuhiro Oikawa, Takeshi Sainoh, Jun Sato
Junichi Nakamura, Yasuhiro Shiga, Yawara Eguchi, Koki Abe
Kazuki Fujimoto, Hiroto Kanamoto, Kazuhisa Takahashi and Kazuhide Inage
Department of Orthopaedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
(Received March 28, 2014, Accepted April 24, 2014)
Purpose. In the current study, we aimed to evaluate the efficacy of PainVision, a tool for assessing the perception of pain in a quantitative manner, for assessing postsurgical low back pain.
Methods. We assessed 42 patients with low back pain after fusion surgery. All patients underwent fusion surgery with posterior instrumented fixation. The numeric rating scale(NRS) score, McGill Pain Questionnaire(MPQ) score, and degree of pain using PainVision PS-2100 were measured twice at 4-week intervals in each patient. For PainVision measurements an electrode was patched on the forearm surface of the patients, and the degree of pain was calculated automatically. The degree of pain was evaluated using both the current producing pain comparable with low back pain and the current at perception threshold. Correlations between NRS and MPQ scores and the degree of pain were determined statistically.
Results. There was a statistical correlation between the NRS and MPQ scores at each time point (rs > 0.56, P=0.001). The degree of pain evaluated by PainVision also showed statistical correlation with NRS and MPQ scores at each time point(rs > 044, P < 0.02). Change in the degree of pain evaluated by PainVision over 4 weeks showed a statistical correlation with changes in NRS and in MPQ scores(rs > 0.4, P < 0.01).
Conclusion. PainVision is useful for assessing postsurgical low back pain.
PainVision, low back pain, surgery, degree, perception
Many tools for evaluating low back pain have been reported. Mostly, self-reported questionnaires have been used to assess back pain. For example, the Oswestry Disability Questionnaire(ODQ) has been one of the most commonly used for evaluating low back pain[1]. The Oswestry Disability Index(ODI) is calculated from the score for each of the ten ODQ items. By contrast, the Roland-Morris Disability Questionnaire (RDQ) was designed for use in primary care research [2]. It has been used extensively in different clinical practice settings(primary care, occupational health, and multidisciplinary rehabilitation centers), to monitor progress in patients with acute, subacute, and chronic low back pain and sciatica[3]. ODI and RDQ scores are dependent on self-reported questionnaires.
In Sweden, up to 25% of patients report unimproved or worse pain and up to 40% are not happy with the outcome of lumbar fusion[4]. There are many possible reasons for poor results, including instrumentation failure, inadequate surgical technique, and poor patient selection[5,6]. Other reported reasons for poor surgical results including presurgical pain/function, negative personality traits, emotional status, anxiety/depression, negative outcome expectations negative coping, duration of back pain, and workers’ compensation[5,6]. In such patients, low back pain is complicated, the objective estimation is difficult.
The scores of the pain assessment questionnaires are based on subjective reporting by patients. PainVision PS-2100(Nipro, Osaka, Japan) has been recently used to quantitatively determine pain intensity as the“ degree of pain” calculated from the electrical current producing threshold perception and the current producing a comparable pain sensation[7,8]. We assessed 89 patients with low back pain, exclusive to patients who had previously undergone spinal surgery and concluded that the numeric rating scale(NRS) score, McGill Pain Questionnaire(MPQ) score, and degree of pain calculated using PainVision were correlated, and that PainVision is as useful for assessing low back pain as self-reported questionnaires [9]
In the current study, we aimed to evaluate the efficacy of PainVision for assessing postsurgical low back pain in patients who underwent posterior fusion surgery with instrumentation.
We obtained informed consent from 42 patients with low back pain and included them in this study. Patients with or without accompanying radicular pain were included. All patients underwent posterior fixation using pedicle screws. The surgical techniques included anterior lumbar interbody fusion(ALIF) with posterior pedicle screws, posterior lumbar interbody fusion(PLIF), transforaminal lumbar interbody fusion (TLIF), and posterolateral fusion(PLF). Presurgical diagnosis was degenerated spondylolisthesis and spinal stenosis, degenerated kyphoscoliosis, and discogenic low back pain. Patients who had infections, tumors, or trauma were excluded from this study.
Low back pain was assessed. Radicular leg pain was not evaluated. The NRS(0-10; where 10 is worst) and MPQ[9](0-45; where 45 is worst) scores, and the degree of pain calculated using the PainVision apparatus were measured twice at 4-week intervals in each patient as previously reported by us [9]. An electrode from the apparatus was patched onto the surface of the forearm of patients, and both the current at the threshold of perception and current producing pain compatible with their low back pain(i.e. the current producing pain of the same intensity as the low back pain as reported by the patient) were measured. The current was pulsed for 0.3 ms at 50 Hz, and 0-120 μA. The degree of pain was calculated automatically(degree of pain= 100×(current producing pain comparable with low back pain-current at perception threshold/current at perception threshold)) (Figure 1). The degree of pain was calculated from the 2 component to one data. The correlations between the degree of pain evaluated by PainVision, and NRS and MPQ scores, and score changes over 4 weeks were evaluated using Spearman's rank correlation test.
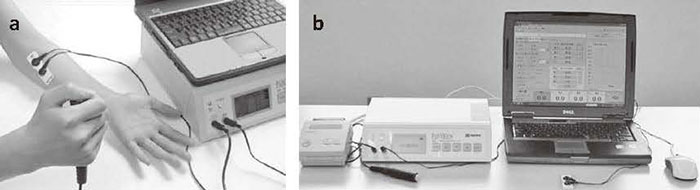
Fig.1 PainVision.(A) Electrodes are patched on the surface of patient forearms, and both current at perception threshold and current producing pain comparable with low back pain are measured.(B) The degree of pain is calculated automatically using software.
Patients were treated conservatively during the 4-week interval between measurements. Medication (only nonsteroidal antiinflammatory drugs) and exercise were allowed at the patient's request. However, surgery was not permitted within the study period.
Data were compared using Spearman’s correlation coefficient by rank test. P < 0.05 was considered statistically significant.
Data in Table 1 show characteristics of the 42 patients before surgery. Patients included those with anterior fusion plus pedicle screws and posterior fusion plus pedicle screws.
Table 1 Demographic characteristics of patient subjects
Correlations between NRS and MPQ scores, and the degree of pain are shown in Figure 1. There was a strong correlation between NRS and MPQ scores(rs = 0.60, P = 0.001). The degree of pain evaluated by PainVision showed moderate correlations with NRS score(rs = 0.50, P = 0.005) and MPQ score(rs = 0.48, P < 0.01).
The correlations between NRS and MPQ scores, and the degree of pain evaluated by PainVision 4 weeks after the initial measurement are shown in Figure 2. There was a strong correlation between NRS and MPQ scores (rs = 0.64, P = 0.001). The degree of pain evaluated by PainVision showed moderate correlations with NRS score(rs = 0.44, P = 0.02) and MPQ score(rs = 0.45, P = 0.01).
Fig.2 Correlation between NRS and MPQ scores, and the degree of pain evaluated by PainVision.(A) NRS score vs. MPQ score.(B) Degree of pain vs. NRS score.(C) Degree of pain vs. MPQ score.
Fig.3 Correlation between NRS and MPQ scores, and the degree of pain evaluated by PainVision 4 weeks after the first measurement.(A) NRS score vs. MPQ score.(B) Degree of pain vs. NRS score(C) Degree of pain vs. MPQ score.
Table 2 Relationship between changes in NRS and MPQ scores, and of degree of pain evaluated by PainVision during 4 weeks

In the current study, there was a statistically significant correlation between the degree of pain calculated using PainVision, and NRS and MPQ scores at each measurement. In this regard, the degree of pain calculated using PainVision is useful for evaluating postsurgical low back pain.
A neurometer may be used to evaluate nerve function and pain objectively in several diseases. Neurometers allow the selective stimulation of nerve fibers with different thicknesses, based on the concept that nerve fibers with different thicknesses have different depolarization times that depend on the frequency of their sinusoid electrical stimulation[10]. Because quantitative electrophysiological diagnosis offers a means by which to evaluate the function of selective nerve fibers, neurometers have been used as auxiliary diagnostic tools for the assessment of allodynia, dysesthesia, and malingering[11]. Several authors have reported that a neurometer is very useful in assessing lower-extremity sensory functions and pain before and after surgery for lumbar disc herniation[12,13]
PainVision PS-2100 has recently been used for the quantitative analysis of pain perception, sensation, and measuring pain intensity[7-9].The PainVision apparatus can stimulate Aβ and Aδ fibers, and the degree of pain is calculated from two variables: current perception threshold and current producing comparable pain[7,8]. A neurometer can only evaluate current perception thresholds; however, PainVision can evaluate the degree of pain automatically by stimulating Aβ and Aδ fibers. Although the patients had low back pain, the electrodes were located on the forearm. The reason is that there are fewer skin hairs and sweat glands, the surface of the forearm is flat, and there is no muscle contraction by stimulation. It has been reported that reproducibility and reliability of the degree of pain obtained from the forearm are significantly superior to those obtained from the foot or leg[14].
There are several limitations to the current study. First, it is relatively small with a restricted number of patients. Second, we did not evaluate psychological factors influencing postsurgical back pain. Further investigation is required to clarify these points.
In summary, we evaluated low back pain after fusion surgery in 42 patient subjects. NRS and MPQ scores, and degree of pain computed using PainVision were measured twice at 4-week intervals in each patient, and we found statistically significant correlations between the 3 types of measurements. We conclude that PainVision is useful for assessing low back pain after surgery.
The authors did not receive and will not receive any benefits or funding from any commercial party related directly or indirectly to the subject of this article.
There are no acknowledgments.
Address correspondence to Dr. Seiji Ohtori.
Department of Orthopedic Surgery, Graduate School of
Medicine, Chiba University, 1-8-1, Inohana, Chuou-ku, Chiba,
260-8670 Japan.
Phone: +81-43-226-2117. Fax: +81-43-226-2116.
E-mail: sohtori@faculty.chiba-u.jp
