




Chiba Medical J. 91E:13~17,2015
doi:10.20776/S03035476-91E-3-P13
[Case Report]
Masahiro Suzuki1), Sumihisa Orita1)*, Takeshi Sainoh1), Kazuhide Inage1)
Go Kubota1), Yasuhiro Shiga1), Kazuyo Yamauchi1), Yawara Eguchi2)
Yasuchika Aoki3), Junichi Nakamura1), Gen Inoue4), Masayuki Miyagi4)
Yoshihiro Sakuma1), Yasuhiro Oikawa1), Yukio Nakata1), Tomoaki Toyone5)
Kazuhisa Takahashi1) and Seiji Ohtori1)
1) Department of Orthopaedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
2) Department of Orthopaedic Surgery, Shimoshizu Hospital, Chiba 284-0003.
3) Department of Orthopaedic Surgery, East Chiba Medical Center, Chiba 283-0826.
4) Department of Orthopaedic Surgery, Kitasato University Hospital, Kanagawa 252-0375.
5) Department of Orthopaedic Surgery, Teikyo University Mizonokuchi Hospital, Tokyo 213-0001.
(Received January 7, 2015, Accepted January 27, 2015)
An 80-year-old woman presented with severe thoracolumbar kyphosis due to spinal tuberculosis with chronic low back pain and gait disturbance. Radiographs showed T9-L1 bony union in the anterior and posterior longitudinal ligaments. Rigid bony union of the L2 and L3 vertebral bodies, with trapezoid-shaped deformity, a sagittal vertical axis (SVA) of approximately 570 mm, and a severe pelvic posterior inclination, were also evident. No residual tuberculous disease was detected. The patient was treated with kyphoplasty, which included an L2 pedicle subtraction vertebral osteotomy (PSO), and T9-S1 fixation. The procedure yielded a 45° correction in the sagittal alignment and enhanced local stability, resulting in an SVA of 50 mm. Her post-operative lower back pain and the gait disturbance resolved. The osteotomy site showed sufficient bony union 8 months post-operatively. PSO yielded marked improvements and stability with no complications such as pseudoarthritis at the osteotomy site. Also her sagittal alignment was corrected to achieve adequate stability with sufficient activities of daily living and improved quality of life. Vertebral osteotomy on those with rigid deformity gives good and stable clinical outcome.
kyphoplasty, spinal tuberculosis, pedicle subtraction osteotomy (PSO)
Spinal tuberculosis is a major form of extrapulmonary tuberculosis, and can result in a severe and rigid kyphotic deformity, with a mean deformity of over 15-60°[1]with approximately 1 to 3% prevalence of all tuberculosis cases. These severe deformities often result in impairments, such as gait disturbance and gastrointestinal disorders, in addition to back pain, due to the malalignment. We describe a case of severe posttuberculous kyphosis, a sequelae of spinal tuberculosis, treated with kyphoplasty.
An 80-year-old woman presented with severe thoracolumbar kyphosis, chronic low back pain with right lower limb pain, and gait disturbance. The latter was due to related symptoms, such as forward head posture. The patient had a history of pulmonary tuberculosis, aged 18 years. The kyphosis was caused by pathological fusion, induced by late-onset spinal tuberculosis at 37 years old. She received no surgical treatment for the spondylitis, resulting in a persistent rigid kyphosis (Figure 1)
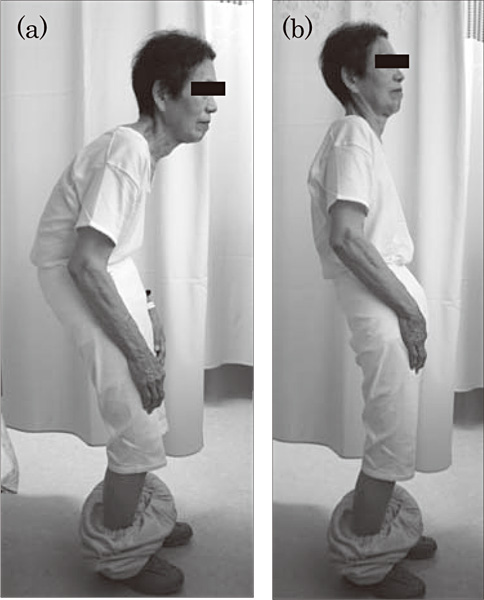
Fig.1 The patient standing in the (a) Neutral and (b) Extended posture. Note that the extended posture is achieved by excessive posterior pelvic inclination.
On visiting our clinic, her low back pain was assigned a visual analog scale (VAS) score of 8-9, after a long gait. Radicular pain in her right lower limb was assigned a VAS score of 8. The patient also complained of occasional reflux or heartburn due to gastroesophageal reflux disease (GERD). Plain radiographs showed T6- L1 bony union in the anterior and posterior longitudinal ligaments, and severe lumbar kyphosis from rigid bony union of the L2 and L3 vertebral bodies, with a trapezoid-shaped deformity. Measurement of the global sagittal alignment parameters revealed the following results: lumbar lordosis (LL)-24.1° (kyphosis); pelvic incidence (PI) 44°; sacral slope (SS)-12°; pelvic tilt (PT) 56°; and sagittal vertical axis (SVA) 420 mm (Figure 2c-d). The measured SVA value was not considered to be a true value, because the patient was unable to stand unsupported; a true SVA of approximately 570 mm was estimated, based on her physique. The sagittal malalignment prevented her from walking on her own and necessitated the use of some mobile aids. Computed tomography myelography and magnetic resonance imaging showed bony union, with partial adipose degeneration of the L2 and L3 vertebral bodies, and L4-5 lumbar spinal stenosis (Figure 3). Vacuum phenomena were noted in the L4-5 and L5-S1 intervertebral disc spaces (Figure 3). The radicular pain in her right lower limb was considered to be secondary to the stenosis. Infection control team physicians noted no residual tuberculous disease. In planning the approach to corrective surgery, we used Schwab’s formula (LL ≤ PI ± 9°)[2], which indicated the ideal restoration for the LL to be 35-53°, requiring approximately 60-80° of LL restoration. To achieve this relatively large correction, we decided to perform a vertebral osteotomy and pedicle subtraction osteotomy (PSO) procedure, with an L3 wedge osteotomy, T9- S1 fixation, and transforaminal lumbar interbody fusion (TLIF) at the L4-5 and L5-S1 levels.
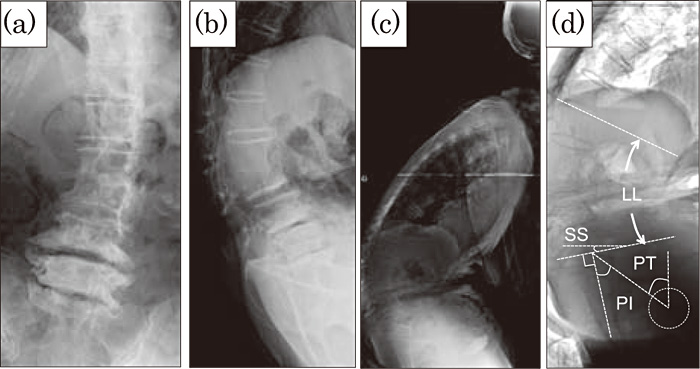
Fig.2 Plain lumbar radiographs. (a) Anteroposterior, (b) Lateral (lumbar), and (c) Lateral (whole spine) images. The patient showed severe kyphoscoliosis. (d) Inversed image with sagittal parameters. LL: lumbar lordosis, SS: sacral slope, PT: pelvic tilt, PI: pelvic incidence (Further details are explained in the text.)

Fig.3 (a) Computed tomography showed posterior components of the thoracic spine showed ankylosing changes. (b, c) Sagittal magnetic resonance imaging. (b) T1-weighed image (WI)(c) T2-WI. Fused vertebrae of L2-3 showed no septic intensity change. No findings related to active tuberculosis were evident.
During surgery, the patient was placed in a prone position. The levels to be operated upon were exposed to the tips of transverse processes (lumbar region) and to the costal attachment (thoracic region), via a posterior midline approach. The hooks and pedicle screws were inserted, and temporary stabilization was performed. The spinous processes showed bony fusion with ossification of the superspinous ligament, thus the most cephalad fusion level was T9, which should be more longer in the usual case. The posterior components of the L3 lamina (spinal process and lower articular processes) and the upper articular processes of L4 were resected, followed by an L3 pedicle osteotomy. An intervertebral cage was inserted to the L3-4 intervertebral disc space, and TLIF was performed at the L4-5 and L5-S1 levels, to offset the instability indicated by the observed vacuum phenomena, and to achieve spinal decompression. There was no need to operate on the L2-3 intervertebral disc, which was already rigidly fused. The surgery took 6 hours 23 minutes, with an estimated blood loss of 1200 mL.
The procedure yielded a 56.1° sagittal alignment correction, and enhanced local stability, with an SVA of 56 mm; LL 32°; SS 26°. Her VAS score for low back pain after walking decreased to 1, and her posture was dramatically improved (Figure 4). Her gait disturbance and GERD-associated gastrointestinal symptoms also resolved. The osteotomy site showed sufficient bony union 8 months post-operatively, and the patient is now able to walk unaided and live independently.
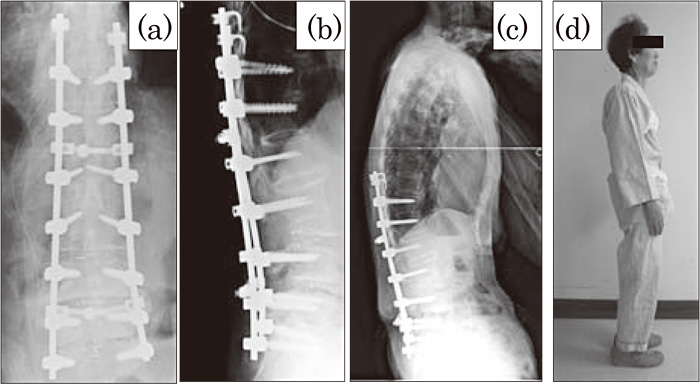
Fig.4 Post-operative radiograph showing effective correction. (a) Coronal plane (b) Sagittal plane (c) Global spinal sagittal alignment was improved with sufficient lumbar lordosis (d) Her posture was dramatically improved with corrected alignment, including normalized pelvic inclination.
Deformities secondary to spinal tuberculosis can result in severe symptoms. Patients treated nonoperatively have an average increase of 15° in deformity; in 3-5% of cases the deformity is greater than 60°. Such deformities can result in complications, including late onset paraplegia and gait disturbance[3,4].
In the standard treatment strategy for spinal tube r culos i s , we should cons ide r pos t e r ior instrumentation and anterior debridement, followed by gross anterior gap grafting and posterior rigid fusion, if the tuberculosis is active[5,6]. Once the disease is cured, the surgical approach can the same as the approach to rigid deformity, such as ankylosing spondylitis, although there are difficulties in terms of routine correction. Also the patients with healed posttubercular kyphosis may suffer with painful costopelvic impingement, reduced vital capacity, and eventually respiratory complications, spinal stenosis proximal to the kyphosis, and paraplegia. Such complications can affect the quality and span of the patient’s life[7]. The present case complained of radicular pain in the right lower limb, ostensibly due to the lumbar spinal stenosis at L4-5.
Regarding corrective surgical procedures, PSO is a useful technique to achieve adequate, reliable, one-stage kyphosis correction, via a posterior approach, to correct fixed sagittal imbalance with middle- and long-term stability[8]. A dorsal osteotomy provides bone-to-bone apposition with inherent stability, and is intended to shift the sagittal vertebral axis dorsally, bringing the spine into balance[9]. Based on these factors, PSO is effective in patients with post-tubercular spinal deformity[10]. The patient presented here had rigid bony post-tuberculous fusion, in which PSO yielded marked improvements in terms of pain and stability.
In this patient, the PSO procedure was also indicated on the basis of the pathology of post-tubercular deformity: Their vertebral column tend to be shortened anteriorly, and the dura mater and spinal cord adjust to the kyphotic position. Therefore, abrupt correction of the kyphosis can result in neurological disorders, due to the enforced lengthening of the anterior column. The shortening of vertebral column achieved with the PSO procedure is desirable, in order to avoid such neurological deficits [5].
A previous study reported that only one third of kyphotic patients reach neutral alignment, even with osteotomy surgery. Considering the possible failure or insufficiency of attempts at correction, in the present case adequate correction and sufficient improvements in activities of daily living and quality of life were obtained[11]. The success of correction in this patient may be related to the relatively small PI; on the basis of Schwab’s formula, a low PI can accommodate a more substantial kyphosis, compared with a large PI [12]. The sufficient correction in sagittal alignment is significant, in that good correction of sagittal and frontal balance enables good clinical and radiologic results that remain stable over time, even when complications occur [13].
PSO is occasionally associated with complications such as bleeding, pseudoarthritis, and instrumentation failure at the osteotomy site; none of these complications occurred in the present case. The procedure corrected her sagittal alignment, achieved adequate stability, and decreased low back pain.
Furthermore less invasive correction surgery using non-osteotomic procedures have been investigated recently. We have already reported a less invasive corrective surgery for severe lumbar kyphosis, using an oblique lumbar interbody fusion (OLIF) technique that includes L5-S1 anterior fusion[14]. A less invasive approach should be considered in such patients.
In conclusion, an 80-year-old woman with severe post-tuberculous kyphosis, presented with gait disturbance, right lower limb pain, and symptoms of GERD underwent corrective surgery with PSO. Her rigid kyphosis was corrected successfully, and sufficient improvements in activities of daily living and quality of life were achieved, without critical complications.
Address correspondence to Dr. Sumihisa Orita.
Department of Orthopaedic Surgery, Graduate School of Medicine, Chiba University, 1-8-1, Inohana, Chuou-ku, Chiba, 260-8670 Japan.
Phone: +81-43-226-2117. Fax: +81-43-226-2116.
E-mail: sorita@chiba-u.jp
