




Chiba Medical J. 91E:29~32,2015
doi:10.20776/S03035476-91E-5-P29
[Case Report]
Takane Suzuki 1)*, Kazuki Kuniyoshi 2)*, Yuusuke Matsuura 2)*
Jun Kakizaki 3)*, Kouji Sukegawa 2)*, Yasuhumi Ogawa 2)*
Tomoko Kobayashi 2)*, Rei Abe 2)* ,Hitoshi Kiuchi 2)*, Keisuke Ueno 2)*
Tomoyo Akasaka 2)*, Aya Kanazuka 1)*, and Kazuhisa Takahashi 2)*
1) Department of Bioenvironmental Medicine, Graduate School of Medicine, Chiba University, Chiba 260-8670.
2) Department of Orthopaedic Surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
3) Division of Orthopaedic Surgery, Chiba Children’s Hospital, Chiba 266-0007.
(Received February 25, 2015, Accepted April 8, 2015)
Syndrome acne pustulose hyperostose osteite(SAPHO) is characterized by synovitis, acne, pustulosis, hyperostosis, and osteitis. Here we report the case of a patient with SAPHO syndrome successfully treated with alendronate. A 34-year-old man presented with a one-year history of recurrent pain at the ulnar side of the right forearm. A roentgenogram and a CT scan revealed the hyperostotic consolidation of the ulna with radiolucent area. Bone scintigram displayed increased uptake at the diaphysis of the ulna, sterno-clavicular joints, and iliosacral joints. Based on these findings, bone curettage was performed. The surgically resected specimen revealed chronic recurrent osteomyelitis, suggesting SAPHO syndrome. We administrated 35 mg of alendronate per week orally. The ulnar pain disappeared for three weeks after this administration. The treatment continued for 13 months, and the patient remained completely pain-free 12 months after the cessation of alendronate. Furthermore, bone scintigrams gradually improved. Alendronate possibly brought initial pain relief through its antiinflammatory effect and long-term pain relief by suppressing bone remodeling.
SAPHO syndrome, bisphosphonate, chronic, recurrent, osteomyelitis
In 1987, Chamot et al[1]reported a syndrome characterized by acne, pustulosis, hyperostosis, and osteitis, which he termed“ le syndrome acne pustulose hyperostose osteite” and abbreviated as “SAPHO.” Thereafter, Benhamou et al[2]included synovitis to the syndrome and renamed it as SAPHO syndrome using the initial of synovitis instead of syndrome. Table 1 shows the diagnostic criteria for this syndrome[3]. The patients with SAPHO syndrome frequently visit orthopedic clinic first because of their bone and joint involvement. Here we describe the case of a patient with SAPHO syndrome successfully treated with alendronate.
Table 1 Diagnostic Criteria for Synovitis, Acne, Pustulosis, Hyperostosis, and Osteitis (SAPHO) Syndrome[3]
A 34-year-old man presented with a one-year history of recurrent pain at the ulnar side of the right forearm. He also had dermatosis for 10 years (Fig.1). The patient’s family history was not remarkable. The roentgenogram showed periosteal reaction (Fig. 2a,b) and the CT scan showed hyperostotic consolidation of the ulna with radiolucent area (Fig. 2c, and d). The ulnar lesion was initially suspected to be a bone tumor; however, biopsied specimen suggested chronic osteomyelitis of the right ulna. Consequently, the patient was referred to our hospital for surgical treatment. A bone scintigram displayed an increased uptake in the diaphysis of the ulna, sterno-clavicular joints, and iliosacral joints (Fig. 3a and b). Blood chemistry showed no abnormalities, including erythrocyte sedimentation rate (ESR), C-reactive protein, and HLA-B27. As a result, we performed bone curettage. The surgically resected specimen revealed a chronic recurrent osteomyelitis, suggesting SAPHO syndrome. Bacterial culture assessment also showed negative results, and finally the lesions observed were attributed to SAPHO syndrome. The patient remained symptomfree for two years after surgery; however, the ulnar pain gradually recurred during the next one-year period.

Fig.1
Dermatosis with acne shown by the patient in his first visit to our clinic
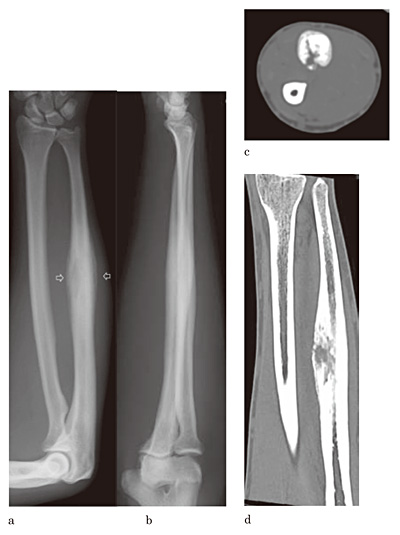
Fig.2
a, b. The roentgenograms of the right forearm showing hyperostosis with periosteal reaction in the diaphysis (arrows)
c, d. The axial and longitundinal reconstructive CT images of the right ulna
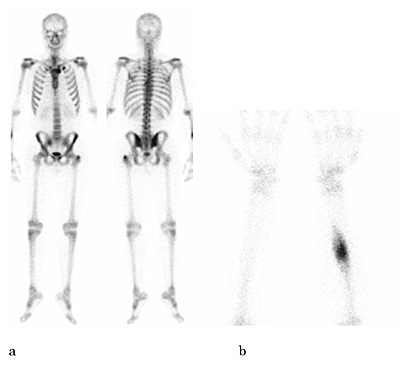
Fig.3
a, b. Bone scintigram at initial examination
The patient used non-steroidal anti-inflammatory drugs (NSAIDs) to manage intractable ulnar pain. No other medical treatment was effective, including antibiotics (minocycline 200 mg or cefotiam 600 mg) or vitamin H. We finally administrated 35 mg of alendronate per week orally, which has been proven effective to reduce the pain. After 3 weeks of treatment, the ulnar pain gradually disappeared. This treatment was continued for 13 months, and 12 months after ending the treatment, the patient continued to report no pain. The periosteal reaction disappeared (Fig. 4a, b). The CT scan revealed moderate hyperostosis with enlargement of the intramedullary canal (Fig. 4c). Bone scintigrams also showed gradual improvement (Fig. 5a, b, and c)

Fig.4
a, b. Roentgenograms at final follow up
c. Reconstructive CT image at final follow up
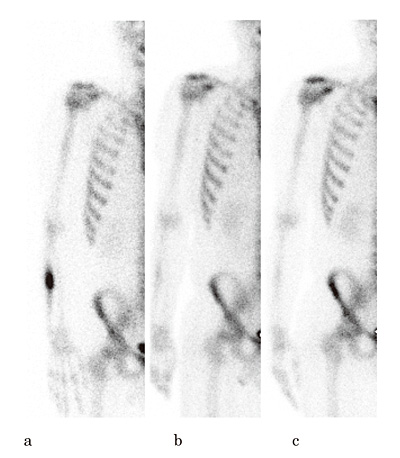
Fig.5
a. Bone scintigram before alendronate treatment
b. Bone scintigram one month before the cessation of the treatment
c. Bone scintigram one year after the cessation of the treatment
Spondyloarthropathy is relatively rare in Japan. Its incidence is reportedly 0.00144 per 100×103 habitants, which is approximately 1/10 to 1/200 of the incidences reported in western countries[4]. Accurate incidence figures from Japan remain unknown; however, SAPHO is likely to be rarer than spondyloarthropathy. Half of the patients presenting SAPHO syndrome also show palmoplantar pustulosis. Hyperostosis and synovitis are also frequently reported at the sterno-clavicular joints, spine, and/or iliosacral joints. SAPHO syndrome sometimes affect long bones of the lower and upper limbs [5,6].
Moreover, the blood chemistry parameters frequently show a slight increase in the inflammatory response without any specific findings. Positive HLA-B27 is reported in 13% of patients with SAPHO syndrome [6]; however, the case described here was negative for HLA-B27. In this case, diagnostic imaging, including roentgenogram, CT, and MRI, revealed hyperostotic changes. Bone scintigrams are also useful in this type of diagnosis for providing a whole-body evaluation. In addition, 18FDG-PET has been reported to be useful to identify active SAPHO syndrome[7]. In the case reported here, a bone scintigram revealed an ulnar lesion and an asymptomatic lesion of the sterno-clavicular and the sacroiliac joints. We often recommend this type of assessment when SAPHO syndrome that is characterized by the involvement of multiple musculoskeletal joints is suspected.
Two hypotheses have been proposed to explain the pathogenesis of the SAPHO syndrome. The first hypothesis involves blood-borne low virulence bacterial or viral pathogens triggering an autoimmune response in the lesion. The second hypothesis suggests a relation with sero-negative spondylo-arthropathies[3]. In the present case, the patient did not show any associated general disease or apparent spondyloarthropathies, except for an asymptomatic sacroiliac joint lesion.
The etiology of the SAPHO syndrome is largely unknown; consequently, the treatment tends to be mainly symptomatic. Current treatment options include NSAIDs, colchicine, corticosteroids, and/or diseasemodifying agents such as methotrexate, sulfasalazine, or infliximab. Other treatments reported included trials involving antimicrobial agents and local corticosteroid injections [8].
Some authors reported the effectiveness of bisphosphonate to treat SAPHO syndrome[9,10] [11]. Our patient was treated with alendronate for 13 months, and although further follow-up checks are recommended, the patient has been symptom-free for one year following the end of the alendronate treatment. Bisphosphonate is an anti-osteoclastic agent used for the treatment of osteoporosis. Furthermore, it has been reported to have anti-inflammatory effects. In addition, Kerrison et al. showed that the anti-inflammatory effect shown by bisphosphonate can effectively suppress the production of interleukin 1, interleukin 6, and TNF-α [12]. They also stated that an acute phase response is usually only observed following the first intravenous administration of pamidronate and is rarely subsequently observed[12]. This type of anti-inflammatory effect could explain the initial pain relief effect shown by alendronate, whereas the subsequent long-term pain relieved achieved by this treatment could relate to the suppression of bone remodeling.
Thus, any anti-inflammatory agents are likely to be effective to treat the symptoms associated with the SAPHO syndrome; however, bisphosphonate may be unique in its ability to achieve long-time pain relief even after the end of the treatment.
Address correspondence to Dr. Takane Suzuki.
Department of Bioenvironmental Medicine, Graduate School of Medicine, Chiba University, 1-8-1, Inohana, Chuou-ku, Chiba, 260-8670 Japan.
Phone: +81-43-226-2017. Fax: +81-43-226-2018.
E-mail: takane.suzuki@faculty.chiba-u.jp
