




Chiba Medical J. 88E:13~18,2012
doi:10.20776/S03035476-88E-2-P13
[Original Paper]
Ichiro Shimoyama1), Yumi Asano2), Atsushi Murata2)
Yoshinori Higuchi3), Tomoyuki Uchiyama4), Hitoshi Shimada5)
Hiroshi Oouchi6,7), Kazuhisa Takahashi7) and Satoru Kuwabara4)
1)Frontier Medical Engineering, Chiba University, Chiba 263-8522.
2)Division of Rehabilitation, Chiba University Hospital, Chiba University, Chiba 260-8677.
3)Department of Neurological surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
4)Department of Neurology, Graduate School of Medicine, Chiba University, Chiba 260-8670.
5)National Institute of Radiological Sciences, Chiba 263-8555.
6)Department of Sports Medicine, Kameda Medical Center, Kamogawa 296-8602.
7)Department of Orthopedic surgery, Graduate School of Medicine, Chiba University, Chiba 260-8670.
(Received November 18, 2011, Accepted December 19, 2011)
Accidental falls may cause serious outcomes for the aged. Motor and sensory systems decay with aging, so reaction time as a placing reflex becomes delay to abrupt changes of the posture. Dynamic postural balance may provide more information than static postural balance. Dynamic postural balance was studied for proprioception of the neck and trunk, and for eyes control. Seven healthy volunteers participated in this study after informed consent. Repetitive alternative rotation of the head(M1) and of the head and thorax synchronized(M2); gazing at a projected point from a laser pointer set on the head, gazing at a fixation point on a screen and closed eyes; comfortable pace(P1) for repetitive alternative rotation, a faster pace than P1, and a slower pace than P1 were asked to do for 20 sec in every combination. A force plate was used for the center of foot pressure, and a wireless 3 axes accelero-meter were set on the top of the head for head motion. Powers were discussed at the same frequency as the head and/or thorax movements. Powers in M2 were significantly higher than those in M1. Neck proprioception should be important than that of thorax for dynamic postural balance.
Postural balance, head rotation, trunk rotation, vestibule-ocular reflex, proprioception
Accidental falls have caused serious outcomes for
the aged[1-3]. Vestibular function, vision[4-7]and proprioception deteriorated with aging[8,9], and muscle
strength and nerve conduction velocity deteriorate with
aging. Motor and sensory systems decay with aging,
sensory-motor feed-back, feed-forward were important,
and vestibulo-ocular and -spinal reflexes work to stabilize
the postural balance[10]. Signals from the proprioceptors
of the muscles and the joints are essential to all the reflexes and volitional movements.
Reaction time as a placing reflex is critical to abrupt
changes of the posture. Dynamic postural balance should
prepare much information, which had been reported for
arm movements[11,12], for rotation on ankles, hips, and
shoulders[13]. Coordination between a neck and trunk
have been reported important between a neck and trunk
[14-17], and between eyes and a neck[18]. Dynamic
postural balance was studied with the volitional neck and
trunk motion with eyes controlled for healthy volunteers.
Seven healthy volunteers participated in this study
after informed consent. They showed no neurological
deficit, aged 43 years(mean) ±11.4(standard
deviation).
Figure 1(Fig. 1) showed a block diagram to measure the
head motion and the center of foot pressure(COP). A
subject was standing upright on a force plate-A(LUB-
100KB®, KYOWA, Japan), 1.2 m apart in front of a
screen. Medio-lateral direction represented as COP-X,
and antero-posterior direction did as COP-Y. Signals
from the force plate were amplified by amplifiers-B
(PCD300A®, KYOWA, Japan), and sampled at 100 Hz
into a computer-C(Pentium IV®). The head movements
were measured with a wireless 3 axes accelerometers-D
(WAA-006® , Wireless Technology, Japan) and the
transmitted signals were received with the computer-C.
The accelerometers-D was fixed on the top of a cap,
and a laser pointer-E was fixed on the brim of the cap.
Another laser pointer-F was set on the thoracic surface. G
was a projected point on the screen from a laser pointer,
and H was a fixation point. Subjects were asked to rotate
repetitively their head only(M1), and asked to do their
head and thorax synchronized(M2). Subjects were asked
to rotate their head or thorax synchronized repetitively
at their comfortable pace(P1), they were asked to do
at the faster pace than P1 by 1.2 times(P2), and they
were asked to do at the slower pace than P1 by 0.8 times
(P3). Subjects were asked to stand still upright gazing
at the fixation point and to do with eyes closed for 20
sec respectively(E0). And they were asked to gaze the
projected laser point(E1) during the repetitive rotation,
and to gaze at the fixation point on the screen(E2), and
were asked to rotate their head and thorax with closed
eyes(E3), on doing M1 or M2, respectively. Subjects
were asked to rotate +/-30 degrees repetitively for
20 sec in every combination. Just before recording the
head motion and COP, P1 was measured for respective
subjects, and subjects were asked to rehearse to rotate the
head or thorax at P1, P2, or P3 for a while.
Recording condition was fixed for all subjects, and
powers were obtained with the fast Fourier transform.
Powers were discussed at the same frequency as the head
motion.
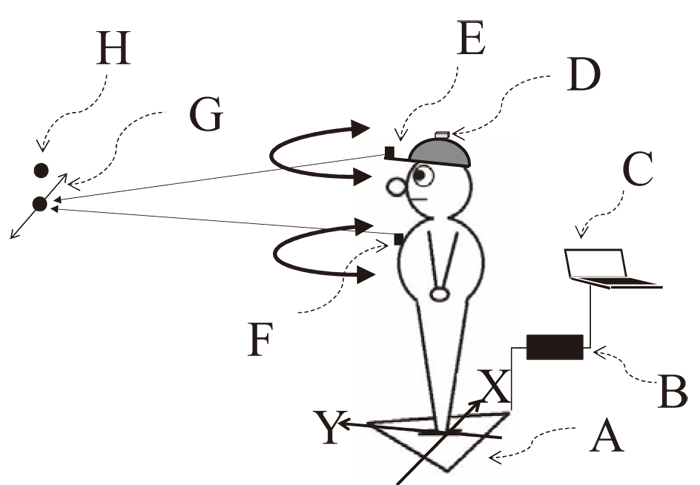
Fig. 1
Block diagram for this study. A was a force plate to record the center of foot pressure, and B was amplifier for the force plate. C was a computer to acquire the head motion and the center of foot pressure. D was a wireless accelerometer to measure head motion. E and F were laser pointers, and G was a projected point from a laser pointer. H was a fixation point. X and Y were directions of the axes for the center of foot pressure.
Mean frequency was 0.5 Hz ±0.05(standard
deviation) for P1, 0.6 Hz ±0.07 for P2, and 0.4 Hz ±
0.05 for P3.
Figure 2(Fig. 2) showed examples of the head position and
COP at P1 for one subject(42 y/o). The head and COP
showed stable enough in standing upright(E0). The
head position oscillated rhythmically at 0.6 Hz for M1
(HEAD) and M2(THORAX), and at E1, E2, and E3.
COP in M2 fluctuated frequently than that in M1, and spectral powers showed increased at 0.6 Hz.
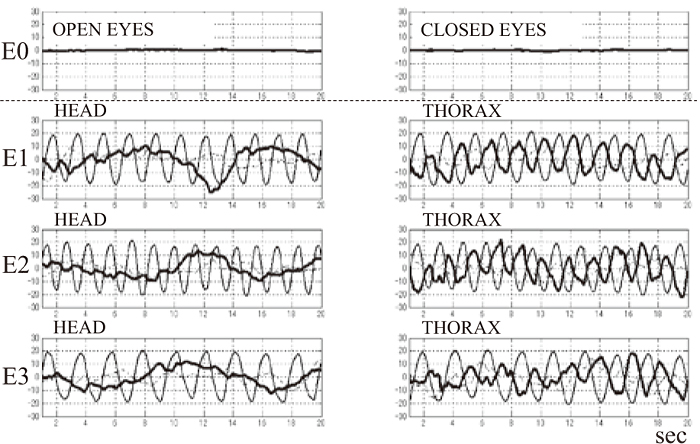
Fig. 2
Examples of the head position and the center of foot pressure at a comfortable pace for one subject, thick traces represented medio-lateral signals, and broken traces did antro-posterior signals of the center of foot pressure. Rhythmical oscillated traces represented the head motion. The abscissas represented time course in sec. A column M1 was for the movements with only the head, M2 for that with the head and thorax synchronized. A row E1 was for the movements in gazing at the laser projected point, E2 for that in gazing at the fixation point, E3 for that with eyes closed, respectively.
Figure 3(Fig. 3) showed examples of the spectral powers for the head motion and COP at P1 for a subject(42 y.) Peak frequency was 0.6 Hz in M1, and 0.55 Hz in M2 for the head motion. Spectral powers at 0.6 Hz showed low at noise level in M1, but powers at 0.55 Hz were noted in M2.
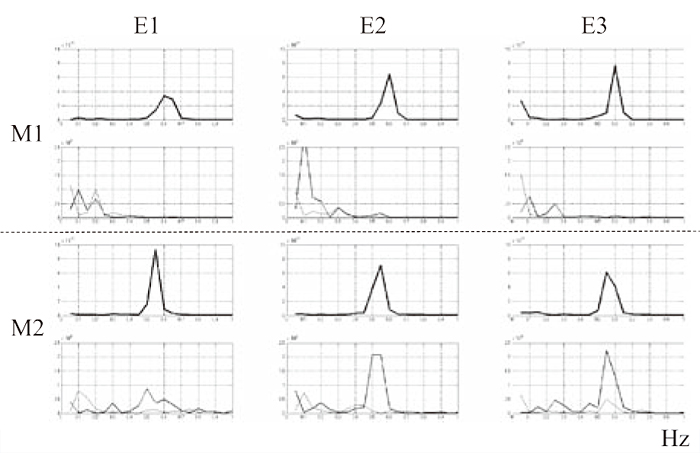
Fig. 3
Examples of the power spectra for the head motion and the center of foot pressure at a comfortable pace for one subject. Upper 2 rows M1 were power spectra with only the head, the uppermost row were those for the movements with the head only, and the second upper row were those for the center of foot pressure. Lower 2 rows M2 were power spectra with the head and thorax synchronized, the second lower row were those for the movements with the head only, and the lowermost row were those for the center of foot pressure. Thick traces for the center of foot pressure were represented for the medio-lateral oscillation, and thin traces did for the antroposterior oscillation. Column E1 represented for the movements in gazing at the laser projected point, E2 for that in gazing at the fixation point, E3 for that with eyes closed, respectively. The abscissas represented frequency in Hz.
Table-1 (Table 1) showed means and standard deviations for the total powers of COP-X and -Y in m²). The analysis of variance showed significant between powers in standing still upright and those in the trunk motion(P<0.005), and no significance was noted between powers with eyes open and closed.
Table 1
Mean and standard deviation for total power

Table-1.
Table showed means and standard deviations of the total powers of the rolling and pich in m². Total powers of the center of foot pressure were significantly higher with trunk movements than those on standing still upright(P<0.005)
Table-2 (Table 2) showed mean powers and standard deviations at the peak frequency of the head motion in m²). The analysis of variance showed significant between powers for M1 and those for M2(P<0.0001), significant between those of COP-X and COP-Y(P<0.001). No significance was noted among powers for E1, E2 and E3, among those for P1, P2 and P3.
Table 2
Peak Powers for Center of Foot Pressure in m²(mean±standard deviation)
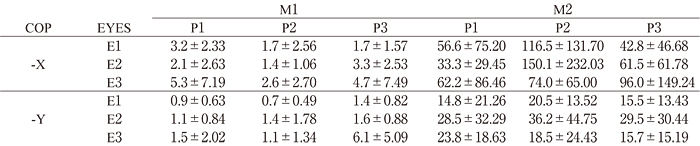
Table-2.
Table showed mean powers and their standard deviations at the peak frequency of the head motion in m². M1 was for the movements with only the head, and M2 was for that with the head and thorax synchronized. P1 was at a comfortable pace, P2 was at a faster pace than P1(P1×1.2), and P3 was at a slower pace than P1(P1×0.8). E1 was for the movements in gazing at the projected laser point, E2 was for that in gazing at the fixation point, and E3 was for that with eyes closed, respectively. COP-X was medio-lateral oscillation of the center of foot pressure and COP-Y was antero-posterior oscillation of the center of foot pressure.
Compensation should keep postural balance stable
for the volitional trunk movements, COP showed
significant oscillation for the repetitive alternative rotation
of the thorax synchronized with the head. Preparatory movements and reflex might compensate for the
volitional movements. The synchronized movements
involved the center of gravity to elicit synchronized
oscillation of COP to keep the stance at the same position.
The mass and weight of the lower trunk need more
energy for the movements than those with only the head.
So COP was easily perturbed for the movements with the
lower trunk. The signals from the vestibular organ were
almost the same for the movements with only the head as
the synchronized movements. The posture was controlled
in standing upright during this study, and the stances
were kept stable. The signals from the vestibular organs
were thought to be consistent. But the signals from the
proprioception were different between those from the
neck or the lower trunk. Visual signals were controlled for
all subjects. The movements with only the head perturbed
COP poor, dynamic energy was less for those with only
the head than that for the synchronized movements.
Range of movements for joints was wider for the cervical
vertebrae than that for the thoracic vertebrae, an odontoid
process is just good to rotate. Repetitive alternative
rotation for the thorax and head synchronized was
equivalent to the motion with the neck immobilized; i. e.,
the proprioceptive signals were inhibited from the neck
in keeping the postural balance stable. Neck motion was
thought to be important to stabilize the postural balance.
A neck had been reported to present much information
[19], and the signals from the neck were of special
importance to positioning the head to the rest of the body
[18,20]. Neck proprioception might be important than that of thorax for dynamic postural balance. The neck
motion has been reported restricted with aging [21,22],
so the aged were used to turn around in rotating the head
with help of the lower trunk motion [3], therefore, COP
was perturbed easily.
There were no differences among the peak powers
at P1, P2 and P3, but compensatory preparatory motion
would thoughtfully be more at P1 and less at P2, and
the sum of the powers at P1 showed minimum for that
of M1 and M2, and of COP-X and -Y, and the sum of
those at P2 showed maximum for that of M1 and M2,
and of COP-X and -Y. The motion at P2 was thought
to be sensitive to keep the balance, so the motion at P2
might be good to evaluate postural balance, because the
variance showed increased.
There were no differences among the peak powers
with E1, E2 and E3, but visual compensation would
thoughtfully work the least with E3 and more with
E1 or E2, and the sum of the powers with E3 showed
maximum for that of M1 and M2, and of COP-X and -Y,
and the sum of the powers at P2 showed maximum for
that of M1 and M2, and of COP-X and -Y. The motion
with E3 was thought to be sensitive to keep the balance,
so the motion with E3 might be good to evaluate postural
balance, but the motion with E3 was dangerous for
the aged, so the motions with E1 and E2 were safer to
evaluate the dynamic postural balance.
Dynamic postural balance at own pace had been
reported for arm movements [12,23], for the rotation on
ankles, hips, and shoulders [24], and for knees [25,26]The method to perturb the postural balance could be
classified into 2 types in studying dynamic postural
balance; one was voluntary movements at own pace
[22,27-29]and the other was unexpected perturbation, i.
e., sudden displacement of any part of a body with outer
force [30-36]. The reports were poor about the repetitive
alternative trunk rotation and COP.
In conclusion, repetitive alternative rotation for the
trunk might present more information than standing
upright still.
This work was supported by KAKENHI(No.23659293), Grant-in-Aid challenging Exploratory Research funded by MEXT, Japan.
Address correspondence to Dr. Ichiro Shimoyama.
Frontier Medical Engineering, Chiba University, 1-33,Yayoi-cho, Inage-ku, chiba city, Chiba 263-8522, Japan.
Phone: +81-43-290-3118. Fax: +81-43-290-3118.
E-mail: ichiro@faculty.chiba-u.jp
